Learning Objectives
This is an intermediate-level course. After completing it,
mental health professionals will be able to:
- Define transference love (TL) and countertransference love (CTL) and the forms
they take.
- Explain why TL and CTL come
alive and how they become operationalized.
- Identify and integrate manifestations of TL and
CTL.
- Summarize steps to take when manifestations of TL
and CTL are suspected.
- Compare and contrast use of transference and countertransference
interpretations with two other ways of managing TL and
CTL.
This course is based on the most accurate information
available to the author at the time of writing. However, cognitive psychology
and neuroscience research on brain development, structures, and activities
continues to shed light on what were once regarded as merely psychoanalytic
concepts and processes. Thus, new information may emerge that supersedes some
explanations in this course. Similarly, new research related to transference
and countertransference interpretations as moderators and mediators of
therapeutic outcome may call for some rethinking regarding their use, their
timing and frequency, and their effectiveness with certain clients.
This course may provoke disturbing feelings in readers due
to the sensitive nature of TL and CTL in
tandem with painful affiliative conflicts readers have not resolved in their
own lives. Guilt, remorse, shame, hate, and envy may be among these disturbing
feelings. If they endure and/or become pronounced, readers may need to seek
supervision, consultation, or personal therapy in order to deal with their
distress.
Outline
- Introduction
- Preparatory Notes
- Why TL and CTL Come Alive in
Therapy
- What Are TL and CTL and What
Forms Can They Take?
- Non-Erotic TL
- Erotic TL
- Eroticized TL
- Perverse TL
- Conditions Affecting the Development of Eroticized and Perverse
TL
- Risk Factors
- Protective Factors
- The Issue of Referral
- How TL and CTL Become
Operationalized in Therapy
- Operationalization: An Overview
- Projection and Introjection
- Projective Identification and Introjective Identification
- Confirmation of Projected Material
- The Healing Potential of Projection and Introjection
- The Human Brain: Its Components and Their Functions
- The Implicit Memory and Schemas
- Similarity Judging: Pattern Matching
- How TL and CTL Are Manifested
- Words
- Emotions
- Dreams, Daydreams, and Fantasies
- Body Language, Complex Movement, and Somatization
- What To
Do with Manifestations of TL
- Overview of Subtasks
- First Subtask: Taking-In Transferred Material
- Second Subtask: Holding and Permitting Regression
- Third Subtask: Decoding and Hypothesizing
- Fourth Subtask: Verifying the Most Likely Hypotheses
- Overarching Meta-Task: Monitoring
- How, Why, and When to Engage Clients in Hypothesis-Testing
- Attitude Required of Therapists
- A Transference Interpretation
- A Countertransference Interpretation
- Qualities of Effective Transference
Interpretations
- Clients Who Can or Cannot Benefit from TRIs and CTRIs
- Timing of TRIs and CTRIs
- Frequency of TRIs and CTRIs
- How to Decide What to Do with TL and
CTL
- The Principle of Abstinence
- Clinical Choices
- Research Findings
- Conclusion
- References
Introduction
Why take this course? Why risk trying to make benevolent use
of phenomena that are inherently dangerous and potentially malevolent?
Why? Because TL and CTL
come alive in non-analytic therapy no less than in analytic therapy. Just
because non-analytic therapists have minimal understanding of them does not
mean that they will lie dormant. Simply put, therapists cannot prevent their
powerful activity during interactions with clients and within themselves (Brenner,
1982). In fact, over the course of time, TL and
CTL will play a major role in most
therapists’ work (Mann, 1999). That’s the bad news.
The good news is that TL and
CTL are double-edged swords. Therapists can make these
inherently transformational phenomena assets. By identifying them,
understanding them, and using them skillfully, they can free their
clients from the bondage of the past for a
future full of wholesome self-love and interpersonal love. By using an
evidenced-based learning process by which clients can develop their capacity
for true intimacy (Schoenewolf, 2004), therapists can make therapy not only
helpful but also benevolent.
This course focuses first on identifying TL
and CTL as they arise, evolve, and become
operationalized in therapy. It then deepens therapists’ understanding
of these phenomena, which are either negative or positive mediators of
therapeutic outcome. It presents theory and research-based guidelines on how
therapists can manage the dangerous aspects of TL and
CTL. Finally, it teaches therapists skills to help clients
meet their affiliative needs through wholesome self-love and appropriate
relationships with others.
A caveat, however, is that this course – in and of itself –
will not make therapists experts in TL and CTL, let alone in analytic thinking. They will not become so knowledgeable and
skillful that they can glide into successful processing of TL and
CTL. No, they will always have to work hard to make
benevolent use of these two ubiquitous and complex phenomena.
This course is the third in a three-part series, based on
the last chapter of a book written in non-analytic language for professionals
with cognitive-behavioral, existential, humanistic, and other non-analytic
theoretical orientations. (Transference and Countertransference in
Non-Analytic Therapy: Double-Edged Swords, by Judith A.
Schaeffer, Ph.D. (Lanham, MD. University Press of America, 2007).
Preparatory Notes
First, each section begins with questions. Taking time to
answer them sets in place a mental schema in which new information can be
accommodated or assimilated in the light of one’s unique clinical expertise and
client population.
Second, because transference and countertransference are
basically the same phenomenon, most of the time the term transference means
both transference and countertransference. Similarly, transference
love means both TL and countertransference
love. Exceptions are made when directly quoting other authors and when the
material would be confusing or misleading if both terms were not used.
Third, efforts have been made to change analytic jargon into
commonly used terms. Because the material in this course is extremely complex, however,
one should expect gradual assimilation of information. This is true partly because
transference and countertransference are interactional phenomena that operate
primarily in the unconscious mind. From the time of Freud in the early 20th century
to the present, theorists and clinicians have struggled to understand and
explain them. They remain challenging.
Fourth, in cases where
gender-specific singular pronouns are used, the masculine and feminine forms
are intended to be reversible.
Fifth, the content of this course is accurate and useful in
that it is based on significant theory and research pertaining to TL
and CTL, beginning in the early 20th century and
continuing into the 21st century. However, the content of this course is
limited by the fact that research pertaining to transference and
countertransference in general and TL and CTL in particular does not always meet current scientific standards. It has
not always been replicated, the number of participants has been low, or there
is no control group. Thus it is not possible to draw firm conclusions
from extant research.
At the same time, it is possible to use this research
to glean valuable information from which treatment decisions can be made
because it is complemented by theory based on a century of clinical practice. Research
findings are complemented by the experience of some of the best clinicians
in the history of psychology, social work, and psychiatry.
Finally, the impact that cultural diversity has on
TL and CTL is short-changed in this course because
of space and time limitations. For the most part, it is left up to the reader
to perform the extremely important task of tweaking information to fit unique
culture-based situations and conditions, both their own and those of their clients. It is crucial, however, for readers to consider dealing with TL and CTL in the context of their clients’ cultural diversity. For example, reaching out and shaking another’s hand may be a manifestation of erotic love in a stereotypic British context but not in a stereotypic Hispanic or Asian Indian context, where it most likely be simply non-erotic and appropriate for all persons or non-erotic but impolite for persons of a higher caste.
Why TL and CTL Come
Alive in Therapy
- What is the relationship between unresolved affiliative conflicts
and TL and CTL coming alive in therapy?
- Why is the human mind so challenged when it tries to detect
TL and CTL?
- Where in the mind do TL and CTL reside?
- What makes the therapeutic setting a likely place for
TL and CTL to come alive?
- If therapists try hard enough, can they prevent TL
and CTL from coming alive in their clinical work?
- If therapists resolve their own conflicts regarding not having
their affiliative needs met, can they expect CTL not to come alive in their clinical work?
- Because therapists know a lot about TL and
CTL, can they regard them as easy to manage in their
clinical work?
- Because therapists are usually quite different from persons their
clients have known, is there really a reason clients see them as individuals
from their past?
TL comes alive in therapy because of what are “kernels of truth,” (DeLaCour, 1985). In the intimacy of the therapeutic
setting, clients interact, usually week after week, with another human being
who bears a resemblance to a person whom they have wanted to love and be loved
by. They were often able to do so with that person but never to the degree to
which they longed. Hence, their mind holds an unresolved conflict.
Then, as clients interact with their therapist, he unintentionally
contributes fragmentary, disguised data that serve as reminders of the original
person. The therapist’s harsh voice, for instance, gives his client subtle reminders
of a verbally abusive parent. The unconscious mind of his client is struck by
sameness, or at least similarity, between the past and the present. The then
and there and the here and now become one reality as the
client finds “an ingenious way to use [his therapist’s] sensitivities” (Hedges,
1992, p. 18). Of course, therapists are vulnerable to doing the very same thing
when their clients remind them of someone in their past.
Freud originally concluded that clients’ transference
elicited therapists’ transference, called countertransference (1912.) Others,
however, discovered that therapists could also elicit clients’
transference because they, too, failed to love and be loved to the extent they
desired. Thus they, too, would have unresolved conflicts and unconsciously transfer
material from them to their clients. Consequently, most theorists now hold that CTL arises both when it is elicited by
clients’ TL and when therapists are the first to send memories to
their clients.
Theorists also hold that TL and
CTL are basically products and processes of the unconscious mind (unconscious). The conscious mind does not intend to produce
them, initiate them, or respond to them. In the case of non-erotic transference
love and CTL, for example, the conscious mind knows the
difference between a therapist and a parent. It is not about to make the past
the present. At the same time, the unconscious, where transferred love resides,
knows only the present. The past lives on as the present (Faulkner,
1929). Thus, we all want to love and be loved in the now.
Furthermore, the conscious and unconscious minds operate
both differently and separately. Their operations are parallel rather than
interwoven. As a result, the conscious mind has virtually no access to what is
in the unconscious. It can only pick up subtle hints of what it contains. Thus,
TL, which hints that it is active in such things as dreams and
involuntary muscle movements, can be detected by the conscious mind only when
it detects these hints, which are termed manifestations.
Vignette:
“My client smiles so sweetly,” the therapist
observed. “She seems to be indicating that she really enjoys our sessions. For
me they are enjoyable also, kind of like sitting at the kitchen table talking
to my mother when I was little. Wish she were alive. She died too early.”
“Great – I am not listening to her. Why is she now
frowning? I guess I’ll have to ask her to ‘tell me more’ so that I cover my
tracks here,” he said to himself. But when he asked her, she grimaced. “Now
what?” he thought.
This reaction of the client puzzled the therapist because
he was not aware of the real issue. The positive reaction he and his client
were having to each other was a hint of transferential and
countertransferential love. He was only aware of having become distracted
because she reminded him of the mother he loved. Likewise, her facial change
was an unconscious manifestation of her disappointment that he had disconnected
from her. “He should not do this,” her unconscious concluded. “My recently
deceased husband loved me so much he never did this. Why did he have to die
before me!”
Indeed, TL and countertransference
love had come alive. They were both outside the awareness of the conscious minds,
but they had uncanny motivational and transformational power.
Notice that in this vignette, TL and
CTL come alive because of stress inherent in an
intrapsychic conflict: one part of the mind contradicting another. This is due
to our experiences as well as to enculturation. In the case of our affiliative
needs, for example, part of us believes we deserve love; part of us does not.
Part of us believes others should find us lovable; part of us does not. Part of
us wants to believe we can be all right without love; part of us believes we
cannot. Part of us wants sexual pleasure; part of us knows that getting that
pleasure, at least with the wrong person, is morally wrong. And so on.
This intrapsychic conflict is both multi-layered and potent.
It causes emotional pain, often excruciating pain. In fact, neuropsychological
research reveals that the human mind is forever looking for ways to resolve
intrapsychic conflict because we fear for our very psychological survival if it
continues (Ecker & Hulley, 1996).
Consequently, clients unconsciously regard therapy as an
opportunity to meet their unmet needs. “I will take advantage of a noticeably
kind, responsive human being who sits across from me,” clients unconsciously say
to themselves. “Yes, this is the perfect time and setting to meet my need to
love and/or be loved. This person will love me, and I will love
him.”
Wanting to experience this love, clients unconsciously
re-enact the past (Covington, 1996). They unintentionally transform their
therapist into a figure from the past – usually a parent but sometimes a
sibling or lover – and assign her the role of loving them and being a person
they can love. They repeat the past; they replay it. They turn passive trauma
into active mastery (Freud, 1912). They “actualize an internal scenario within
the therapeutic relationship that results in the [person they are with] being
drawn into playing a role scripted by [their internal role]” (Westen &
Gabbard, 2002, p. 101). They make their interaction with their therapist an
“adventure from which [they] hope to emerge changed and renewed” (Cooper, 1987,
p. 518).
This happens easily because the therapy setting bears striking
resemblance to early prenatal and/or natal experiences.
Think about it. Except for multiple births, we are alone in the
warm, safe womb. We are enclosed, protected from the external environment
(Laplanche, 1997), and given all that we need. We are even “waltzed around & set
in motion, always accompanied by the rhythmic beat of a mother’s heart,” (Elise,
2019, p. 29). Then, when born, we are kept warm, dry, fed, and shielded from harm.
We are picked up, held, and carried. Someone else does for us what we cannot do
for ourselves.
So it is in therapy. Clients find themselves in a safe,
“warm” environment where a person focuses intently on them, then “picks up”
their ideas and “carries” them forward. This person mirrors what they say and
comments on what they know but cannot put into words. Thus they feel validated,
cherished, and nourished with the “food and drink” of unconditional, positive
regard. They begin to feel loved as a mother/father-figure lightens their pain
by holding it alongside them.
In the case of TL, clients gradually perceive
that structures have been put into place whereby they can meet their long-lived
affiliative needs. Seemingly incongruent things have come together. They may
have to take some responsibility for resolving their intrapsychic conflict, but
in the “womb” of the therapeutic setting, another person has already functioned for them and with them. They have been loved. They can
risk believing that they are lovable. They can risk expressing and receiving
love (Covington, 1996).
In other words, what they have yearned for in the past, can
finally be achieved because they have unconsciously displaced the present with
the past yet experienced it as the present. They have engaged in transference
love and found it matched by CTL.
Yes, therapists unconsciously enable TL to
come alive by “allowing” their own CTL to arise. They
unwittingly both open themselves up to receiving their clients’ transference
love and transfer their own TL to their client. They try, on an
unconscious level, to resolve their own affiliative conflicts. In no time,
unconscious bidirectional collaboration has occurred without it being
consciously willed.
Furthermore, more often than not, in the case of non-erotic
transferred love, both clients and therapists alternate roles. Like a
kaleidoscope, “one moment the therapist is seen through the lens of the
parental figure and the next” (Diamond, 2018, p. 411) through the lens of the infant (Diamond, 2018, p. 411).
It is the same with the client as both therapist and client unconsciously try
to meet the totality of their affiliative need: loving and being
loved.
In sum, TL arises when clients perceive their
therapist as someone from their past and thus transfer love related to an
unresolved affiliate conflict from the past to the present. Countertransference
love arises when a therapist does this.
Fortunately, what usually comes alive in therapy is
non-erotic. However, love that is non-erotic can become erotic, eroticized, or
perverse.
What Are TL and CTL and What Forms Can
They Take?
What are the forms in which TL and
CTL arise in therapy?
- What form of TL or CTL is
likely to come alive initially in clinical practice, given the population a
particular therapist works with?
- Should non-erotic TL, which is so innocent, get
much attention?
- Do therapists really need to detect and manage erotic
TL in light of its being such a positive human experience?
- Might therapists safely rule out eroticized TL in
their clinical practice in light of their professional ethics and their having resolved
their own affiliative conflicts?
- Because perverse TL can be thought of as subhuman
and in the mind and heart of just a few individuals, might it be regarded
as having no value in life, let alone in therapy?
- What are the client-related conditions under which eroticized and
perverse TL are likely to become operationalized?
- What are the conditions under which therapists themselves might
enable eroticized and perverse CTL to become
operationalized?
- What protective factors lower the probability of TL
and CTL causing serious problems for clients and for
therapists?
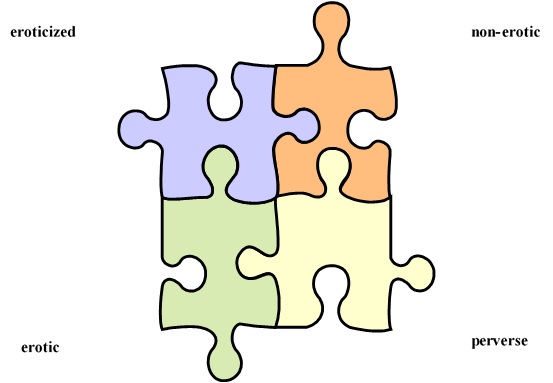
TL takes four basic forms: non-erotic,
erotic, eroticized, and perverse. These forms overlap but have unique
characteristics. We begin with one that is far from pathological. In fact, it
is a mediator and moderator of human development: non-erotic TL.
Non-Erotic TL
Freud (1912) believed that non-erotic TL is
both intrapsychic and interpersonal. It is grounded in the innate human need to
give love to and receive it from another person.
Meeting this affiliative need is essential to human well-being not only in the
womb and after birth but also throughout childhood. Indeed, it is essential to
some degree throughout life.
We focus on unresolved affiliative conflicts with maternal
figures in this course for the sake of brevity and simplicity. But this is not
intended to underestimate the presence and power of other affiliative
conflicts, starting with paternal and extending into sibling, friend, and
significant other. Affiliate conflicts with all of these can and do trigger
non-erotic TL in therapy because no interpersonal relationships
completely satisfy human affiliative needs, let alone desires and longings. The
result? Intrapsychic conflict.
Because we are finite by nature but virtually limitless in
our expectations, early attempts to meet affiliative needs are both positive
and negative. For most of us, our basic needs are met. But they are not met well
enough. We are loved but not fully, not consistently, and not flawlessly. Yet
we feel we have a right to it. Hence, we unwittingly endeavor to resolve the
conflict between what we have received and what we believe we were and still
are entitled to (Freud, 1912).
Non-erotic TL is a matter of our unconsciously re-enacting
our early years so that new, positive experiences can replace painful memories
of this conflict. We perceive empathic, understanding individuals as potential
nurturing mother figures (Freud, 1912; Covington, 1996). We “seek intimacy,
which ordinarily includes bodily contact, with those we experience as warm and
accepting” (Schaeffer, 2007, p. 187). We want them to provide for us satisfying
reparative experiences by acting in such a way that we know we are
loved because we feel loved. We replace pain in the past with
gratification in the present.
Thus, it is normative for non-erotic TL to
come alive in multiple and various interpersonal settings: in therapy and
outside of it, for therapists as well as clients, for mental health
professionals as well as other providers.
The therapeutic setting, however, is especially conducive to
this happening. Even in the first session, therapists extend unconditional
acceptance, positive regard, and sustained benevolent interest in clients and
what they share. Consequently, clients perceive their therapists as kind, caring,
nurturing, and loving persons with whom they can enter into a whole-person,
non-erotic, but gratifying relationship. Put succinctly, therapists become
longed-for mothers, and therapy becomes an opportunity for clients to find
vanished mother figures (Ferenczi, 1909).
Correspondingly, clients become longed-for infants and
children because of their vulnerability and willingness to depend on their
therapist, whose profession consists, in part, in acceding to the emotional
demands of others (Hedges, 1992). The therapy room becomes an ideal setting for
intimate contact through conscious and unconscious channels of communication
(Tower, 1956) and the therapeutic process, an opportunity for therapists to
nourish and nurture clients into new life. Thus therapists and clients enjoy
the mother-infant quasi-union of the first months of life (Greenacre, 1954).
In Jungian terminology, the therapy room is a natural
setting for the Mother Architype to become operationalized. Therapists see it
as an opportunity to play maternal roles (Schaeffer, 2007) as their clients
transfer their love for their biological mother to their therapist. Therapists’
unconscious enactment of their non-erotic CTL allows
clients to conclude – also unconsciously – that the love they have transferred
has been accepted. Alternately, it seems to them that they have every reason to
transfer that love because they are already loved. All will go well. They will
finally meet their affiliative needs.
Indeed, when all goes well, non-erotic TL is
similar, if not identical, to non-erotic love outside the therapeutic setting.
It is satisfying. It is fulfilling. That is the good news.
The bad news is that for those who are no longer infants or
children, psychological maturation is a matter of integrating one’s capacity
for self-nurturance and self-love into the psyche, rather than depending solely on
being nurtured and loved by others (Ferenczi, 1909; Freud, 1940). In other
words, adults must meet their affiliative needs primarily in
and through themselves and only secondarily in and through others. Sole
or even primary dependence on others is no longer developmentally appropriate.
Thus, TL proves not to be
the panacea clients expect. The resolution of early-life affiliative conflicts
is no longer possible simply because they receive non-erotic love
from others. They also need to give it. And ironically, the therapeutic setting
gives them an opportunity to do so because both male and female therapists fall
quickly and naturally into taking on maternal roles and performing nurturing
functions (Greenacre, 1954). They resonate with weak, vulnerable, and virtually
helpless individuals needing their non-erotic love. To simple empathy and a
caring attitude, therapists add affection for those hungry for love and for loving
responses.
Their clients, in turn, welcome those expressions of love,
for they believe they cannot heal from their affiliative pain unless they
experience a phenomenon first described by Ferenczi: “It is the physician’s
love that heals the patient” (Gerrard, 1999, p. 29). Alternately, it might well be
the client’s love for the therapist that heals, which is what Freud (1974, pp. 8-9)
meant when he wrote: “Essentially, one might say, the cure is effected by love”
(Charles, 1999). Or it might be both. In any case, that’s the good news.
The bad news is that as much as non-erotic TL
and CTL are beneficial during the therapeutic process, both
can become liabilities. Even if they stay non-erotic, they can distract
therapists and clients from focusing on the maturational work needing to be
done. If they morph into the erotic, they add a new, very challenging dimension
to already difficult therapeutic work. And if they become eroticized and/or
perverse, both clients and therapists can be overwhelmed by powerful feelings
and the impulse to act on them.
At the same time, of course, these developments can give
clients and therapists an opportunity to work on a deep and meaningful level,
rather than a more comfortable though “arid and superficial” level (Charles,
1999, p. 258). By addressing the most crucial needs of the human heart, they can
make therapy truly beneficial.
Erotic TL
Erotic TL is a matter of clients “[falling]
in love” with their therapist (Rabin, 2003, p. 677). It is a non-pathological form
of sexualized love. It is clients’ normal sexual response to a certain person
outside therapy being transferred to their therapist. Erotic
CTL is the same: therapists’ loving their clients in a
non-pathological but sexual way.
The feelings clients and therapists have for each other are
as genuine as they would be in a non-therapeutic setting (Slavin, et al.,
1998). They are also as natural and real as those of non-erotic transference
love (Celenza, 2017).
Erotic TL begins as non-erotic (Freud, 1912).
Like all positive human dynamics, it can be traced to an early erotic source: a
sensual mother-infant relationship. “The early mother-infant bond is the first
erotic relationship” (Schaverien, 1997, p. 10). Erotic TL stems
from the infant’s spontaneous, primitive need to feel wanted and loved and to
experience love physically. “Affectionate attachments from early childhood are
retained in the personality through puberty, when they become enmeshed in an
individual’s sexuality” (Hedges, 1992, pp. 18-19). The maternal-infant relationship
“is maternal eroticism” (Elise, 2019, p. 29). The relationship of the mother to
her infant can even be termed primal seduction (Laplanche, 1997).
In other words, erotic TL is as normative in
therapy as non-erotic TL. Sexualized TL and
sexualized CTL trigger each other (Dalenberg, 2000)
because of our universal vulnerability as human beings (Celenza, 2021). Moreover,
erotic TL and non-erotic TL tend to vacillate
rapidly (Slochower, 1999).
Erotic TL is “genetically linked with
sexuality and develops from purely sexual desires through a softening of their
sexual aim” (Wrye & Welles, 1989, p. 5). Sensual pleasure easily gets
“interpreted” as sexual because sexual desires lay at the deepest level of the
human psyche. The needs from which they arise are as basic as those for food,
drink, and sleep. Thus, both the conscious mind and the unconscious mind are
ever alert for opportunities to fulfill sexual desires and meet sexual needs.
Furthermore, because human beings tend “to experience
themselves as unlovable at a very deep level” (Mann, 1999, p. 19), they
instinctively search out others who will make them feel lovable.
They are determined to meet their affiliative needs. Correspondingly, others
are motivated to meet those needs, showing them “once and for all that [they]
are really loved” (Celenza, 2017, p. 159). And the most convincing proof of doing
so is providing a sexual experience, at least in the “opinion” of the
unconscious mind.
The unconscious mind is far more “experienced” than the
conscious mind because it is a much older evolutionary development. Thus it is
more able to motivate behavior than its younger partner.
Furthermore, it is easy and natural for sensual experiences
to become sexual in the human psyche because the unconscious mind does not make
a distinction between the body and the mind, as does the conscious mind. The
latter “says” that there are differences between a person’s physicality,
mentality, emotionality, and spirituality. The unconscious mind, in contrast,
“says” that the mind must use bodily organs to function and therefore emotions
and sensations are simply “two sides of the same coin.” Each emotion is felt as
a sensation or a cluster of sensations. Each sensation or cluster of sensations
automatically sends a message that an emotion or emotions are being
experienced. Thus, feeling warm, comforting sensations “means” to the body that
it is in proximity to someone who has positive, if not loving, feelings toward
it.
Additionally, the unconscious mind makes no distinction
between thinking and feeling because the one cannot help but accompany the
other. It feels good, for example, to read the loving message on a valentine,
even as feeling loved is automatically accompanied by the thought “I am loved.”
Furthermore, in the unconscious mind an emotional-cognitive
experience of intimate love is also physiological. “When we touch another
person, we do not just touch a body, we touch a being" (Celenza, 2017,
p. 160), and vice versa. Emotional warmth and loving thoughts and words are
simultaneously experienced as tender, loving bodily contact.
Put succinctly, the unconscious mind does not buy into the
mind-body duality “claim” of the conscious mind. As a consequence, in the human
psyche, lines between fact and fantasy easily fade. Similarities become
sameness.
Thus, closeness evolves into enmeshment. Separateness morphs
into merger. Then, in an effort to meet its sensual-sexual or erotic needs, the
unconscious mind engages in transference. It displaces love for an early-life
individual to an individual in the here-and-now. In the therapeutic setting, clients
unconsciously conclude that their therapist is a mother who truly loves them.
Moreover, they truly love their mother-therapist. Therapists, in turn,
unconsciously conclude that their client is one whom they love, one whose
affiliative needs they must meet (Hedges, 1992), and one who
is able and willing to meet their own affiliative needs.
In other words, erotic TL and
CTL is ignited by both therapists and clients (Schaverien,
1997), by men as well as by women (Silverman, 2019). Both bring to the
therapeutic endeavor an erotic unconscious (Mann, 1999) and an erotic vulnerability
(Celenza, 2021).
Erotic TL occurs naturally in therapy because
during its course, therapists reveal things about themselves simply because of
what they say and how they say it. Clients share sensitive information about
themselves, and therapists open themselves to highly personal information about
their clients. Indeed, clients’ tendency to discuss sexual material in therapy
is a common characteristic of clients to whom therapists are attracted (Pope,
et al., 1994).
Thus, it is common for both clients and therapists to
feel something more (Dalenberg, 2000) than the non-erotic. It is the erotic: a
combination of liking, having loving feelings, fantasizing desired sexual
experiences, and falling in love (Rabin, 2003). It is a combination of the
pleasure of mutual love and the “pleasure [of] proximity, [the] desire for
fuller knowledge of [another person], [and a] yearning for mutual
identification and personality fusion” (Menninger, 1942, p. 272).
Keep in mind, however, that transferring erotic love is
not intentional. It is simply a matter of two individuals
unconsciously allowing their imaginations to produce a fantasy of being loved
and loving the person who loves them (Mann, 1999).
At the same time, there are actually “kernels of truth” to
this fantasy because although the conscious mind is unable to detect
TL itself, it is sensitive to manifestations or signs of it.
They may be subtle and highly disguised, but they are detectable. The look in
the eye of one who loves another erotically, for example, is inherently
different from the one who loves another non-erotically.
Jung (1946) adds an interesting observation that explains
why erotic TL is not uncommon in therapy. At a deeply unconscious
level, he says, erotic transference not only connects clients and therapists in
a fantasy, but also allows clients to find wholeness. They seek a therapist
because they are broken and splintered. They have split from an
unlovable-unloving part of themselves. They want “to be reconnected to a
missing part of themselves, to some aspect of their own souls,” adds Jungian
analyst Ulanov (1984, p. 76). They hope to reconcile with a split-away part of
themselves: the one that they are transferring to their therapist.
Seen in this light, erotic TL, like
non-erotic TL, is far from pathological. Indeed, it evolves from
a willingness to share control of a relationship that blends love with other
human feelings, aspirations, and needs. It is a complex phenomenon that
integrates both aggressive urges and sexuality with love and tenderness
(Gabbard, 1989). It brings with it ever-shifting feelings of love, shame,
idealization, envy, rage (Davies, 1994), and even hate (Blum, 1997).
As a general rule, erotic TL first engenders
shame and embarrassment, for both therapists and clients are aware of cultural
and moral prohibitions against their fulfilling their erotic desires with
socially inappropriate, unavailable individuals. In addition, the contract
therapists make with their clients is to maintain a boundary between therapy
and external life (Morris, 2012), between a therapeutic relationship and a real-life
relationship. They will work to understand the client’s deepest human desires,
but not fulfill them. They will gain insight, but not act on it.
In time, however, as therapy becomes more demanding, even
painful, it is neither uncommon nor unnatural for therapists and clients to
desire relief. They want to experience the pleasures of acceptance and
appreciation along with intimacy and endearment. Thus they unconsciously
bring about a relationship that permits experiences of love for one another as
whole persons: human beings with intimacy desires, sexual needs, and sexual
impulses. They no longer want to relate just intellectually or even just
emotionally and/or spiritually. They want to act on what they feel, that is, to
relate physically.
Put succinctly, erotic TL takes form “at the
interface where mental and physiological experiences come together” (Davies,
1994, pp. 158-159). It is no wonder then that as non-erotic TL fuses
with pleasure that is erotic, it quickens in both clients and therapists strong
urges to take advantage of opportunities to gratify sexual desires (Etchegoyen,
1978). In spite of multiple prohibitions, the therapeutic setting becomes an
opportunity for clients and therapists to meet their affiliative needs at the
deepest level. They fantasize that a loving, sexual experience will enable them
to love and feel loved. They will finally resolve a painful, foundational
affiliative conflict they have endured for a long time.
In sum, erotic TL is a normal, whole-bodied,
physiological, emotional-sensual-sexual phenomenon that is normative in a
therapy setting. If carefully managed, it can be used to enable clients and
therapists to work together to meet their affiliative needs in mature,
fulfilling ways in real life. They will no longer be conflicted over the fact
that “they should not want what they haven’t got – a message often received
from those with too little to give” (Charles, 1999, p. 249). That’s the good news.
The bad news is that the therapy setting is fraught with
danger. Erotic love can evolve – and can do so insidiously – into eroticized
love and perverse love. Furthermore, when undetected and unmanaged, it can lead
to immoral, unethical behavior.
Eroticized TL
Eroticized TL is a pathological displacement
of love. It is clients’ unconscious attempt to heal their painful, negative
memories of not being satisfactorily loved by expressing their attraction to
their therapist in one or more forms of purely physical sexual behavior
(Gabbard, 1994).
In the past, clients have experienced rejection from those
whose love they sought. Now, they unconsciously fantasize that by acting out
sexually with their therapist, they can fulfill their desire for intimacy. As
they express their love physically, a sense of goodness will replace a sense of
badness (Slochower, 1999). Their self-esteem will increase exponentially
(Stacy, 1998). Gratification of sexual desires will replace their quest for
understanding and being understood, which are the very heart of therapy (Freud,
1915). “All other deep unconscious wishes will prove superfluous in the light
of all-consuming sexual gratification” (Schaeffer, 2007, p. 190).
Eroticized TL is pathological because it is truncated.
It consists of sexual components alone (Person, 1995). In contrast to mature,
seasoned love, it makes sexual gratification the end-all of interpersonal
relations. Commitments to others are meaningless.
Eroticized TL that appears in early stages of
therapy tends to result from clients’ frustration over not having the control
they want over their therapy and their therapist (Eickhoff, 1998). In other
words, eroticized transference serves as a defense against fears of
helplessness and feelings of powerlessness. By contrast, eroticized
TL that arises at termination is usually a defense against the
pain of being separated from the therapist they have come to love.
There are then at least three possible outcomes to eroticized
TL coming alive in therapy. The benevolent, indeed very benevolent,
one is that therapists detect it and manage it skillfully and thereby help
their clients meet their affiliative needs in developmentally appropriate,
person-appropriate ways, outside the therapeutic setting.
A clearly malevolent outcome, by contrast, is that
eroticized TL ignites subtle but powerful rescue fantasies that
therapists fail to detect. They can then be seduced into meeting their clients’
sexual needs by enacting their own eroticized countertransference. Sadly, in
spite of years of ethics courses and information from professional associations
and state grievance boards, engaging in sexual activity with clients remains
one of the main reasons therapists lose their license. They deny their
responsibility to those outside of therapy. They break their covenant with
their clients, betray them, and lose their trust. No matter how gratifying the
experience in the short run, they grievously damage their clients as well as
their own families (Celenza, 2021).
Another, though less malevolent, outcome is that eroticized
TL makes therapists feel captured and bound rather than free to
love. They experience a negative form of sexualized countertransference. They
want to disconnect from clients they perceive as intensely needy, demanding,
and self-centered. In that case, the clients come to realize how misguided their
efforts to force love have actually been. They experience painful masochism.
And their therapists experience shame and guilt related to their professional
work.
These two malevolent outcomes would be the same, of course,
if it were the therapists’ eroticized TL that began the
process.
Perverse TL
Even more pathological than eroticized TL is
perverse TL, for it is actually a form of hate (Stoller, 1975).
It is the hate once inflicted on the client by an abusive or neglectful other
and now projected into the therapist as the client unconsciously reverses roles
and becomes the abuser. Perverse CTL is pathological for
the same reasons.
Verbal signs of perverse TL are hostile
provocation, sarcasm, outright rejection of the other person’s ideas, and
forcing one’s own on them. Paradoxically, emotional coldness can be a
manifestation of perverse transference. In any and all cases, “perverts [are]
not making love; [they are] making hate” (Kaplan 1991, p. 40). They are
sadistically reducing another person to an inanimate object that can be used,
abused, and then discarded at will. There may be no physical contact in the
therapy setting, but the verbal and/or nonverbal behaviors of one individual
make the other feel humiliated, violated, and exploited. Consequently, aversive
emotional confusion soon debilitates both of them (Slochower, 1999).
Perverse TL is characterized by compulsivity,
fixation, rigidity, and obligation (Kaplan, 1991). Those who engage in it have
little if any choice. Their hatred is so deeply entrenched, and they understand
it so little, that they can neither recognize it nor control it. Rather, they
feel compelled to protect themselves, by acting out, from what they sense will
lead to their own psychological destruction: their hatred of another (Springer,
1996).
In rare cases, perverse TL can take an
alternate form. As one individual “grooms” another, they adopt an attitude of
extreme, unfailing kindness (Gabbard, 1994). They normalize intimate exchanges
in such a way that sexual material is inserted into their relationship without
being noticeable. Even so, well informed and skillfully observant recipients of
perverse TL will periodically perceive those who transfer it as
children who have been painfully abandoned or abused. They are powerless individuals
whose frightening emotional pain compels them to protect themselves against
further abandonment and abuse by seducing those with whom they are presently
interacting (Springer, 1996).
Blum (1997) perceives perverse TL in another
way. He sees it as a sexualized defense against hate, hostility,
humiliation, a desire to destroy, and a fear of being destroyed. It is a
defense against the pain of having been deserted or abandoned – actually destroyed psychologically
– in the early years of life. Those transferring perverse love are
unconsciously hoping to seduce another person instead of being seduced.
Blum (1997) explains further that those who displace
perverse love are unconsciously attempting to fulfill their desire to take
revenge (Springer, 1996). By enacting this form of love, they are hoping to
eliminate – or at least be separated from – another person. Their seduction, be
it real or imagined, will make the other individual into an impersonal object.
Thus they will be saved from being rejected by a real person whom they actually
love (Khan, 1979).
Beneath the attempt to be saved from rejection by being the
first to take revenge is a devastating affiliative experience (Russ, 1999).
Hence, in the therapeutic setting, a therapist’s first and foremost endeavor
must be to endure transferred feelings of hate long enough to experience that
experience of the client. The biggest mistake the therapist could make is to
refuse to deal with perverse love, for that would almost inevitably confirm the
client’s “conscious or unconscious belief that his sexuality and aggression
either sullies or violates” (p. 611) both him or her and the therapist. There
would be no solution other than to despair. In contrast, daring to stay with
perverse love long enough to deal with it can lead, later rather than sooner,
to the “deep contact” (p. 611) that permits a person to hope for healing.
Springer (1996) contributes yet another useful theory. He
believes that, at the deepest psychological level, perverse TL
is a sexualized defense against the self. It gives the one who enacts it an
experience of pseudo-wholeness and completeness, which is extremely exciting.
Thus, it protects the individual from experiencing psychological
disintegration. If one is experiencing overwhelming excitation, he or she
cannot be disintegrating. Hence, the powerful reinforcement that propels serial
rapists into repeated offenses.
Finally, Mann (1997) points out that perverse transference
love is a desperate attempt to connect to another human being. It is an effort
made by one person to relate to another for the sake of resolving an extremely
painful affiliative conflict. Hence, those initiating it feel compelled to find
one person after another to relate to. Hence the serial rapist.
What might therapists contribute to their client’s perverse
TL? Nothing, we hope. But let us not forget that the phenomenon
of transference depends on one person being open and willing to receive the
transference from the one displacing it. As therapists begin to feel the burden
of their therapeutic work – especially if they do not lead a balanced,
wholesome life – their anger and aggressive urges can taint their maternal
erotic CTL. It can even disappear in the face of growing
dislike or actual hatred for their client (Schaeffer, 2007). It can lead to
therapists meeting their own sexual needs with their client, violating the
contract they have made with them to keep the therapeutic setting a safe place
to share the most personal aspects of oneself. For therapists have promised “to
maintain [their] awareness of separateness [from their clients] and inhibition
of [their] own desires and needs” (Celenza, 2017, p. 159). They have promised “to
forego cultivating, expressing, and acting on what [they] might personally
desire” (Celenza, 2017, p. 161).
It is frightening but true that therapists who act out their
eroticized and perverse CTL can unconsciously believe that
they can discharge their disguised archaic instincts with impunity. They can
hold the delusion that they can give sexual expression to their hatred and
hostility without causing harm (Bachant & Adler, 1997).
On the other hand, identifying and talking through eroticized
or perverse TL can be extremely beneficial to clients. Doing so
says to them that although their desires will not be acted out because of the
harm that would bring, they are accepted and valued. Aspects
of them perceived as vile do not make them vile. Instead, they
can process the painful affiliative experiences that have spawned a
pathological form of love. They can reject it instead of incorporating it into
their sense of self. Indeed, therapists who do not deal with
their clients’ eroticized or perverse TL make their professed
unconditional love “a mere platitude” (Charles, 1999, p. 260).
Conditions Affecting the Development of Eroticized and Perverse
TL
Risk Factors
Under certain conditions, the probability of eroticized and
perverse TL and CTL developing is high. A
distinction is being made between TL and countertransference
love even though they are interdependent and thus co-occur.
Client-related conditions under which eroticized and
perverse TL are more likely to develop include:
- Clients with pronounced psychological injuries from early and
intimate experiences may both desire and fear intimacy. They may act out with
an empathic therapist (Chodorow, 1978; Schaverien, 1997).
- Clients who have experienced repeated and/or grievous sexual
abuse may fuse sexuality with affection. They may want to substitute action for
painful remembering (Schaffer, 1997), most often by playing the role of the
aggressor themselves (Kernberg, 1994). Conversely, they may want to make their
therapist play the role of a potential aggressor who chooses not to
abuse them (Schaeffer, 2007).
- Clients with a pronounced histrionic personality structure may
want to attack a therapist they idealize but find insufficiently responsive to
them (Kernberg, 1994).
- Clients with a deep-seated dependent personality structure may
fear being engulfed and thus annihilated by their therapist
(Chasseguet-Smirgel, 1984). They may “feel dependent on the [therapist] while
passive-aggressively thwarting all efforts to help,” (Shedler, 2021, p. 10) until
they become so distressed that they act out.
- Clients with a pronounced narcissistic personality structure may
want to prove how powerless a therapist who appears powerful actually is (Nissen, et al., 2020; Tanzilli, et al., 2017).
- Clients with strong masochistic tendencies and a long history of
unhappy love affairs may want to express their feelings of sexual inferiority.
- Clients whose parents used cruel, passive-aggressive ways of
expressing their hostility may find it natural to imitate these methods.
- Clients who have been socialized to be overly compliant in terms
of meeting others’ needs may want to meet their therapist’s needs (Celenza,
2017).
Therapist-related conditions under which eroticized and
perverse CTL are more likely to develop include:
- Therapists with longstanding and profound guilt feelings may want
to be punished for their transgressions (Kernberg, 1994). They may
unconsciously believe that pursuing what is clearly forbidden will bring them
that punishment.
- Therapists with pronounced narcissistic tendencies may want to
enact their powerful rescue fantasies (Kernberg, 1994). They may unconsciously
believe that by being sexual with clients who crave sexual expressions of love,
they will save their clients from those desires. Especially prone to do this
are therapists who are extremely needy because they are grieving over such
experiences as an unwanted divorce or an endangered clinical practice. This is
especially true of those who have not disciplined themselves to say “No” to
themselves (Celenza, 2017).
- Therapists with strong masochistic tendencies who treat highly
seductive narcissistic clients may want to make up for the inadequacies of
other people in their clients’ past (Jacobs, 1986).
- Therapists with strong characterological impatience may want
their clients to achieve a full sense of relatedness and thus be angered by the
distance their clients keep from them (Smith, 2000). Especially if they feel dismissed
by their clients, they may try to assuage their painful feelings through sexual
closeness.
- Therapists with pronounced proclivities toward envy may want to
side for or against their clients, especially adolescents, with regard to their
sexual freedom (Kernberg, 1998).
- Therapists with omnipotent healer strivings or a sustained savior
complex may want to overcome the resistance of clients who try to thwart them.
They may throw their sexuality onto the balance in an effort to fulfill their
mission (Searles, 1979).
- Therapists with perfectionistic tendencies who put therapeutic
tasks ahead of maintaining the therapeutic alliance may not attend to
manifestations of problematic transferred love.
- Therapists who are depleted may not be able to replenish the energy
they have lost in the course of their clinical work (Celenza, 2017).
Needless to say, if clients who have suffered from trauma
and/or present with profoundly problematic characteristics meet with impaired
therapists, the danger of their acting out is significantly higher. It may even
be exponentially higher. That’s the bad news.
The good news is that protective factors can be put in
place.
Protective
Factors
Protective factors that reduce the likelihood of clients and
therapists enacting pathological forms of TL and
CTL include:
- Clients who enjoy a supportive adult relationship outside of
therapy may find the other a person with whom they can meet their affiliative
needs.
- Clients who have developed a wholesome lifestyle may find their
therapeutic work less stressful. They may be able to detect, early on,
transference processes they need to disclose to their therapist. They may easily
muster the courage to do so.
- Therapists who have resolved their own sexual and aggressive
conflicts may detect dangerous transference processes early on. They may have
the psychological freedom to address them benevolently.
- Therapists who have developed a wholesome lifestyle may find
their therapeutic work either less stressful or relatively easy to recover
from. They may easily access the professional skills they have developed.
- Therapists who participate in their own therapy during periods of
more-than-usual stress may be able to process early on their own contribution
to TL becoming problematic.
- Therapists who get supervision or consult with colleagues may
more easily identify transference phenomena and thus take steps to use them
benevolently (Celenza, 2021). They may be able to allow their “own erotic
response, including attendant emotions, to become available for discourse with
[clients who transfer to them eroticized and perverse love]” (Russ, 1999, p. 605). Especially helpful in supervision is the use of literature to discover TL and CTL. Research findings reveal that discussing literature provides “a safe and nonjudgmental, almost ‘therapeutic,’ environment where therapists, particularly trainees, can encounter their own feelings, process those feelings, and reflect on those feelings, without immediate clinical consequence” (Lewis, 2024, p. 5).
Vignette:
The client wasn’t particularly pretty, but her
occasional fun-loving flirting was charismatic. In time, her therapist noticed
how much he looked forward to her sessions and how he thought much more about
her than his other clients. Finally, he became aware of sexual feelings toward
her, the same feelings he enjoyed while dating his ex-wife. He also realized that what
was happening to him was becoming a problem. Worried about this, he decided to
tell his client that she had made enough progress to try going on her own. They
didn’t need to continue to meet.
Fortunately, through consultation with a colleague,
the therapist realized what he was actually doing. He was avoiding dealing with
his CTL by convincing himself and his client that they
could terminate. As a consequence, at the beginning of their next session he said
to her, “I find myself attracted to you,” he said. “But I’m trying to push it
under the rug by suggesting we end our work. Could it be that the flirting you
initiate, and we both enjoy, might be working against us?”
“Perhaps,” she replied sheepishly. “I just can’t
feel good if a man isn’t in my life in a sexual way. Actually, more than one
man, because I’ve had affairs while married as well as when divorced.”
With this disclosure, the client and her therapist
were able to explore her affiliative needs. They eventually did much-needed trauma
work regarding her need to act out early sexual abuse.
The Issue of Referral
Therapists with protective factors in place need not
terminate with clients when TL becomes problematic. In fact,
doing so can imply that clients are neither honorable nor respectable, neither
moral nor ethical. They are disgraceful because of their disorder, impairment,
or immaturity. It would be too difficult, if not impossible, for their therapist
to help them resolve their affiliative conflicts.
Instead, what these clients actually need is acceptance as
individuals in dire need of help to meet their affiliative needs in wholesome
ways. They need a therapist they can trust enough to share their affiliative
pain.
Exceptions exist, of course, but rarely can a therapist
determine clients with whom they cannot profitably work when TL
first arises. In fact, the majority of clients respond well to boundary-based
acceptance by therapists who show them how to put protective factors in place
while both they and their therapist take responsibility for their behavior.
Indeed, most clients benefit immensely from being respected as individuals
whose basic affiliative needs are legitimate and whose capacity to meet those
needs in mature and responsible ways can be developed.
How TL and CTL Become Operationalized
in Therapy
- What unconscious processes enable TL and
CTL to be operationalized in therapy?
- Why do these processes occur repeatedly in spite of therapists
knowing about them and being motivated to keep them from affecting their work?
- Why does the unconscious mind put pressure on the human psyche to
engage in unconscious processes that enable TL?
- How is projective identification different from projection? And
why does projective identification tend to bring about greater relief than
projection?
- How likely is it that both therapists and clients will engage in
projection and projective identification?
- What accounts for the affiliative conflicts that clients project
not automatically becoming a negative experience for their therapist? Or becoming
so?
- How is introjective identification different from introjection?
And why does introjective identification tend to inflict more distress than
introjection?
- What is the healing potential of projection and introjection in
and of themselves?
- How does the structure and functioning of the human brain relate
to TL and CTL?
- How are schemas and pattern matching related to TL
and counter-TL?
- What can therapists do to counteract the potential of
operationalized TL to wreak havoc in therapy?
Operationalization: An Overview
TL and CTL come alive in
the therapeutic setting just as they do in life in general. Their doing so – in
and of itself – is benign. If they become operationalized, however, they gain
the power to either re-wound or bring about healing.
TL and CTL come alive
when a client or therapist unconsciously transfers affiliative material either
onto or into the other person. If the material is put onto the
other person, the process is called projection; if into the
other person, projective identification.
For the process of projection to be completed, the other
person must take on or take in the material being transferred.
Taking on or simply receiving the material is called introjection;
taking it in is called introjective identification.
Operationalization depends on whether the person
taking on or in the material confirms it; identifies with it in the sense of
owning it. Operationalization is a two-step process.
Projection and Introjection
The first step is one person projecting – displacing or transferring – some aspect of his unfulfilled affiliative desires
or unmet affiliative needs onto another person and the other
person introjecting or receiving/taking on what is projected. These aspects may
be feelings, sensations, thoughts, behaviors, or a combination of them.
What is sent must be received/taken on. Likewise, what is
received/taken on must be being sent. In the case of TL,
therapists can only introject the love that their client projects. In the case
of CTL, clients can only introject the love that their
therapist projects. If that does not happen, the displaced material simply returns
to the sender.
The projection-introjection is done by the unconscious minds.
When clients and therapists project TL, they do not realize that
they are doing so. They do not even recognize what they are projecting as their
own. It feels foreign to them. But it is conflictual and therefore painful:
some kind of love that should have been reciprocated but was not. They deserved
love but did not receive it. They tried to love another person, but their love
was unrequited.
The unconscious knows only the here-and-now: the present. It
does not know the there-and-then: past (or the future, for that matter). Thus an
affiliative conflict that has in fact arisen in the past and outside the
therapy room is experienced as occurring in the present and in the room. “My therapist/client
is a person who loves me and/or is receiving my love,” the unconscious of the
one projecting “says” to itself. “My affiliative conflict is being resolved.”
Similarly, the unconscious of the one introjecting “says” to itself, “My
client/therapist is a person whom I love and/or whose love I am requiting. Her
affiliative conflict is being resolved.”
Projective Identification and Introjective Identification
Projective identification and introjective identification
can be thought of as mutations of projection and introjection; they take them
“a step further” (Shedler, 2021) and “deeper.” Projective identification is a
matter of one person unconsciously putting material into another. Introjective
identification is a matter of another person unconsciously permitting that
material to enter into her (Ogden, 1982). Thus, projective
identification and introjective identification push the psyche of the one
introjecting to complete the displacement process. It becomes harder – though
not impossible – for the person not to do so.
Projective identification occurs because the human psyche
fantasizes that it can split off a painful – and thus undesirable – part of
itself by putting it into another person. Later on, it can recover a
modified, non-painful version of that part (Grinberg, 1997; Ogden, 1982). In
fact, while the one who receives the material holds it, the one who has sent it
experiences a oneness with the recipient (Schafer, 1977).
Projective identification occurs because the human psyche unconsciously
knows that it needs to learn how to deal with the past
(Schore, 2003a). It needs to discover how to manage the unresolved conflictual
pain it has thus far been unable to get rid of. Thus a client suffering from
depression resulting from not being loved puts her unmanageable sadness and
hopelessness into her therapist. Then she observes what her therapist does with
those feelings.
Ideally – and this word is very important to remember – she
notes how her therapist momentarily stops talking in order to calmly consider
what words might match his feelings. Far from denying his distress or letting
it overwhelm him, he is calmly preparing to describe it. He is collaborating in
the projective identification process by internalizing the hopelessness and
sadness inherent in depression. Observing this, the depressed client gets
relief. Her therapist is depressed. She is not.
Furthermore, she is learning a new way to deal with
depression caused by unmet affiliative needs or desires: verbalizing it calmly
rather than denying it or letting it overwhelm her. As a result, her depression
is manageable (Ogden, 1994). She can now safely re-own her sadness and
hopelessness. She can recover the part of herself she has put into her
therapist.
This does not always happen, however. What is being put on
or into a person is not necessarily confirmed or owned by the one taking it in
or on.
If one engages in simple introjection – takes on a
projection – his unconscious immediately “reports” that there is something
superficially wrong with him, such as “I don’t love others.” If he engages in
introjective identification – takes in a projective identification – his
unconscious “reports” that he is inherently defective, saying “I cannot love
others.” In other words, if an unconscious message is delivered “with …vehemence,”
the person receiving it is pressured to “feel and act in accord” with the
message (Shedler, 2021, p. 23).
Thus introjective identification usually results in a deeply
disturbing and often visceral experience. Introjectors “describe experiences of
not being able to think their own thoughts or feel their own feelings, as if
their minds have been colonized by something alien” (Shedler, 2021, p. 23;
Gabbard, 1994). Therapists “may find themselves filled with hatred for their
[clients] or impelled to cross professional boundaries to rescue them.
Observable behavior…pulls, pushes, coaxes, and coerces [therapists] into their
assigned roles” (Shedler, 2021, pp. 23-24). The same is true of clients.
Confirmation of Projected Material
Those who introject material that has been projected do not
necessarily own it or identify it as theirs. They cannot help but feel what
the projector has felt, but they do not necessarily make that feeling their own
or agree that it is factual or true. They do not have to confirm
it (Schafer, 1977). They can choose not to identify with it or own the
feelings, thoughts, perceptions and sensations connected with it (Stamm, 1995).
Confirmation of a projection depends primarily on whether or
not recipients have resolved their own intrapsychic conflicts related to what
they have introjected (Westen & Gabbard, 2002). It depends primarily on
“the extent to which the…projection meshes with aspects of [their]
unresolved…conflicts” (Meissner, 1996, p. 43).
For example, if a client projects onto a therapist a hateful
mother figure, if the therapist has not resolved
her own affiliative conflict of loving as well as hating her own real-life
child, she will confirm the projection. She will identify with, authentically
feel, and own the “label” she is receiving. And she will tend to take the role that
matches the label. As a result, she will enact her hate, perhaps by being
emotionally unresponsive. She will withdraw. She will not listen empathically,
if she listens at all, or soothe her client. She will move on even though her
client is beginning to cry. She may even express her hate by disparaging her
client.
Contrastingly, if a therapist has resolved her conflict of
loving as well as hating her own real-life child, she
will be unlikely to confirm her client’s projection of her as a hateful mother
figure. She will not own the “label” her client gives her. She will not take
the role of a hateful mother-figure.
If a therapist confirms negative projections of what she
introjects, she is likely to create serious problems in the course of providing
therapy; problems for herself no less than for her clients. For example, she
will experience guilt. Then, in all likelihood, that guilt will prompt her to
make amends. She might try to express love in ways that should convince the
client of her love but will not be appropriate in a clinical setting. Being
hugged or kissed, for instance, may comfort or satisfy a client at the time,
but in the long run it harms him (Celenza, 2021). It sends him the message that
his therapist is willing to love him as would a mother of an infant.
What is equally problematic is that the therapist will not
be conscious of what she is doing at the time she is doing it. Only later will she
realize the full impact of her actions. Before she becomes aware of how she has
tried to meet her client’s needs, she will have harmed him.
Conversely, the more a therapist has resolved her
affiliative conflicts, the higher the probability she will not confirm
what she has introjected. Rather, she will use it to design appropriate
interventions that mediate and/or moderate a positive outcome.
It is difficult, however, for therapists and clients
to completely resolve conflicts related to affiliative needs
because the human psyche wants to be loved perfectly and to
love others perfectly. Thus, when experiences in therapy are
less than perfect, both therapists and clients fail to find them authentic, let
alone convincing. They tend to reject them and judge each other to be as guilty
as were persons outside of therapy and in their past (Schaeffer, 2007). Even if
therapists and clients perform close to satisfactorily, they will
be condemned for not doing so perfectly. They will have added “insult to
injury.”
It is no wonder, then, that Freud concluded back in 1912
that processes called transference and countertransference could
never really resolve intrapsychic conflict and bring about lasting healing. In and
of itself, acting on displaced material could not make up for past experiences
of being unloved or unable to love or finding one’s love unrequited. Only understanding
them and learning how to meet affiliative needs in the present could heal a
person.
Unfortunately, however, the human brain is primed to engage
in projection and introjection, along with projective identification and
introjective identification, in an effort to get relief from painful memories
or relieve someone else of them. Furthermore, it is primed to confirm the pain
another psyche sends it in an effort to heal it by taking away its pain. Thus, both
clients and therapists feel compelled to process emotional pain (Schore, 2003a).
They are “wired” to remember what happens to them. They are physiologically and
psychologically programmed to bring past unresolved affiliative conflicts into
the present and expect them to be resolved by that alone. Thus, completing the
process of TL and CTL is not surprising.
But is it adaptive? Does it work?
The Healing Potential of Projection and Introjection
Do these processes heal persons in and of themselves?
No. For when individuals introject material, one of two things happens. They
either come to feel like those doing the projecting and become empathic toward
them. Or they come to feel like the original recipients of the material and
empathize with them. In the case of a depressed person, for
example, it would be the people being affected by that individual’s sadness,
hopelessness, lack of energy, and other symptoms. In the case of anger, it
would be victims of the angry person’s verbal abuse.
Then, if a therapist feels empathic toward a client, healing
may be underway. If not, the client experiences even more pain; once again not
being understood and having affiliate needs unmet. That is the bad news.
However, it is good news if the therapist manages
transference and countertransference effectively and thereby gains important
information regarding what a client has contributed to his interpersonal
problems and what she herself contributes to her own problems. She has learned
about her client’s failure to deal with what he has
contributed to his unmet affiliative needs. She can then use this information
to provide client-specific interventions that will address exactly how her
client might change his interpersonal interactions. If she has learned what she
has contributed to her own unmet affiliative needs, she can use the information
to improve her own interpersonal interactions.
This is not easy, however, because of the components and
functions of the human brain.
The Human Brain: Its Components and Their Functions
Because of the human brain’s limbic system’s amygdala, it is
always storing emotionally charged events, such as experiences with caregivers.
Because of the brain’s limbic system’s hippocampus, it is always tagging time
and place to affiliative memories so that they can be stored as narratives
(Schore, 2003b). Because of neuromodulators that encode memories, the human
brain is always in the process of forming painful memories of not being loved
and failing to love others. Because of neurotransmitters that activate reward
centers, the brain is always in the process of trying to get rid of emotional
pain simply by experiencing the love of others.
Furthermore, because of the human brain’s mirror neurons, it
reacts to someone else being loved simply because it is near that person. Thus
clients and therapists are automatically and unconsciously communicating with
each other as soon as there is activity in one of their brains. “You are my
loving mother,” the client’s brain “says,” whereupon the therapist’s brain,
which is just a few feet away, receives information regarding his or her
maternal assignment and the role he or she is being told to perform (Schaeffer,
2007).
The Implicit Memory and Schemas
In addition, because of the brain’s implicit memory, it
constantly stores and recalls what it learns experientially. It continually encodes
and generalizes feelings, sensations, and images of what happens. Thus they are
available when there are similarities between the past and the present. They
serve as natural “building blocks,” making the present temporarily
indistinguishable from the past and the therapeutic setting indistinguishable
from a setting outside of therapy.
Cognitive theorists think of generalization as schema-making.
Schemas tend to “proclaim” the beliefs within them. Thus they “encourage”
transference and countertransference (Gabbard, 2001). “Mothers are emotionally
cold even though I need to be loved,” proclaims a schema in the memory of the
unloved child. “This is exactly what my therapist, who looks like my mother, is
going to do,” proclaims the schema-making brain in the same, though adult,
client. “I must reject this client who appears to need too much love,” proclaims
the introjected schema in the therapist’s brain. “My whole body tells me not to
be emotionally responsive to her.”
In other words, a client’s schemas serve as templates
that can be imposed on new reality not only for them but also for their
therapist. Should a therapist confirm and then enact the schema,
it becomes an even more compelling belief in the unconscious of the
client.
Matters are even more complicated because one schema builds
upon the other. “Old schemas never die; they…are incorporated in various ways
into subsequent schemas.” They are “periodically activated without conscious
awareness,” (Westen, 1998, p. 331) as human needs activate similar
information-processing channels.
What becomes problematic then in the course of therapy is
that schema-nesting gives clients and therapists the opportunity to transfer
their intrapersonal and interpersonal struggles to each other. Neural pathways
of schemas remain intact even though they may be weakened or even made
temporarily unusable. “Although perhaps inhibited, [neural networks] are
capable of reactivation in certain circumstances” (Grigsby & Stevens, 2000,
p. 97). That’s the bad news.
The good news is that recent research of Ecker, Hulley, &
Ticic (2012) suggests that certain interventions can weaken, even destroy,
neurons and neuropathways that have encoded toxic schemas.
Similarity Judging: Pattern Matching
TL and CTL can also be
thought of as repetition and re-enactment due to similarity judging: pattern
matching. The human brain is continually constructing and reconstructing
experiences in the context of old ones. Thus new interpersonal experiences are
understood in the context of old ones. “Transferential processes always reflect
an integration of current and past experience, as patterns of activation
resulting from current life experiences…interact with enduring ways of
responding” (Westen & Gabbard, 2002, p. 130).
It may seem as if human beings just “take in” the world as
it exists – as does a camera – but in fact their perceptions are constructed by
their brain (Gazzaniga, 1995). Acting like a feature detector, the brain uses
already existing sensory cues based on prior experience to see and hear and
feel what it saw and heard and felt before. It “searches for a match between
the current [or present] pattern of neuronal activation and patterns stored in
memory [because of prior experiences]” (Pally, 1997, p. 1021). It finds patterns
within itself. It makes “a quick assessment of just enough details to find a
‘good enough’ match. When one is found, perception occurs” (Pally, 1997,
p. 1025). We “see” what we have seen before. Thus, we transfer the past to the
present. That’s the bad news.
The good news is that TL that results from
similarity judging need not result in negative outcome. If therapists perform
subtasks that detect and manage it, they can “exploit transference for its
optimal learning potential…. They can thereby convert a potentially…dangerous
perceptual “mistake”…into an opportunity to adopt new, more effective patterns
of meeting their own and [their clients’] affiliative needs” (Levin, 1997,
p. 1147).
How TL and CTL Are
Manifested
- Why is it so difficult to detect TL and
CTL as it is becoming operationalized?
- Why must therapists detect TL and countertransference
love and do so as early as possible?
- Why might therapists mistake manifestations of transferential
love as simple pieces of information that clients are conveying? Why might
therapists misidentify manifestations of their own CTL?
- What guidelines should help therapists from erring either on the
side of ignoring manifestations of TL or becoming overly
suspicious of what is transpiring in therapy?
- What are some categories of manifestations of TL?
- Which manifestations of TL are easier to detect?
Which are more difficult?
- What might therapists need to do with those which are difficult?
Because of an all-but-impenetrable barrier between the
conscious and unconscious minds, the conscious mind cannot have direct
knowledge of phenomena “residing” in the unconscious mind (unconscious). As a
result, the conscious mind can detect transference only in the vague, shadowy
signs of its presence. It can be identified only when it manifests itself in
dreams, slips of the tongue, connotative language, sensations, emotions, body
language, and behavior. For each of these “voiceless and vociferous little
parts of [the self]…do their best to add their ‘two cents’ into the final
product” (Wittig, 2002, p. 143): truly meaningful communication.
As an intrapsychic phenomenon, communication is from an individual’s unconscious to the individual’s conscious
mind. The communication occurs because the two minds need to “talk” in order
that the more logical conscious mind can work with the more emotional
unconscious to resolve conflicts. Without the contribution of the unconscious,
the conscious mind is not likely to deal effectively with life’s challenges
(Schaeffer, 2007). It is not likely to resolve its affiliative conflicts.
As an interpersonal phenomenon,
transference is a matter of two individuals’ unconscious and conscious
minds communicating. The communication is a matter of subtle, indirect
manifestations rather than clear, direct information. Nevertheless, the reason
for the communication is the same as it is for the individual person: the four
minds need to “talk” in order that the more logical, analytic conscious minds
can work with the more emotional, intuitive unconscious minds to resolve
conflicts.
This work is very difficult because manifestations of
transference cannot be taken at face value. They are sources of data regarding
what is going on in therapy but not sources of evidence of
exactly what it is (Smith, 1990). They must be unpacked “to the point of their
yielding the truths they hold” (Schaeffer, 2007, p. 65).
This is especially true regarding the cultural variables
inherent in manifestations of transference. Therapists must pay attention to
their transcultural as well as within-cultural meanings. In a Hispanic culture,
for instance, transferred maternal love is generally quite different from that
in a British culture.
In the process of transferring its contents into the
conscious mind, the unconscious uses a variety of ways. The following
categories of transference manifestations are artificial in one respect.
Emotions, for example, find expression in words, sensations, facial expressions.
But we will examine the categories separately in order to simplify complex
phenomena and create templates that can be used in therapy.
Words
Words used in therapy might simply be means of communicating
the problems and concerns clients and therapists are aware of. If so, they can
be taken at face value, that is, according to their dictionary definitions or
denotations.
Even so, some words not only convey straight-forward
messages but also carry emotional overtones, connotations. For example, a
client calling her biological father abusive may be unconsciously
referring to all men as abusive.
Therapists should likewise suspect countertransference with
words they sometimes choose, especially those that come “out of the blue.” “I’m
afraid I can’t give you an appointment next week,” may also mean “I am afraid of
hearing more about your sexual issues and therefore do not want to schedule
you.”
Words spoken at the beginning or end of sessions are
especially noteworthy in terms of transferred meaning. A client who walks in
saying, “I am so tired of trying to relate to my unloving partner,” may also
mean “I am tired of trying to get you to love me.”
Words that convey seemingly unrelated material may also be
transferential. When talking about a third party, clients may be unconsciously
revealing their feelings about their therapist. “I feel so attracted to my
boss,” for example, may also refer to the therapist. It may not, of course,
which is why it is very important to examine possible manifestations of
transference.
Emotions
Though single, obvious emotions would not appear to be
transferential, what appears to be simple may be complex, with a second or
third emotion at the periphery of the obvious emotion. Anger that a client
expresses when talking about her husband, for example, may also include sadness
because the therapist, like the husband, is not available as a lover.
Theorists vary as to which emotions are most likely to be
transferred. But because clients and therapists want to bond with each other,
love and fear of disappointment should be expected. Similarly, when therapy
goes well, relief is often accompanied by fear of therapy coming to an end and
thus a loving person disappearing from one’s life. In fact, the earliest
bonding experiences commonly consist of a positive experience of needs being
met on demand, followed by a negative one of learning that one has asked too
much and/or too often (Schaeffer, 2007).
When decoding emotions, therapists must also consider body
language and voice quality. The meaning of words can change dramatically if
gestures or tone of voice or volume do not match the words. “I feel comfortable
in here,” said with strained facial muscles and in an almost inaudible tone of
voice, most probably means, “You make me comfortable, but I need more from you.”
In general, therapists first discover the truth about their
own transferred emotions in those emotions which seem excessive or
inappropriate for what clients say or do (Tower, 1956). Therapists’ sudden
anger, for example, simply because their client is a few minutes late is most
likely excessive. Indeed, therapists’ reactions, be they sensations or
emotions, are typically based on already existing affect or physiological
states. Their becoming angry might be based on their guilt related to disliking
a client (Schafer, 1997) despite their belief that they should not dislike clients.
Their becoming nauseated might be based on their anger with clients who talk in
circles (Racker, 1968). Their sleepiness might be based on their already
feeling abandoned by clients who habitually intellectualize.
Arlow (1985) theorizes that the depression therapists have in
spite of their healthy lifestyle and overall professional success is basically
a countertransferential reaction; a defense against the depression of their
clients. More often than not, clients project a bad self (Epstein, 1977;
Racker, 1968) onto or into their therapist because of similarities to prior
caregivers. What is equally problematic is that therapists whose own
self-definition is negative may unconsciously add self-punishment to negative
transference. They may “agree” that they are inadequate (Epstein, 1977), for
example, because they find it almost impossible to work with clients with endless
affiliative needs.
The fear that therapists sometimes develop in their clinical
work may be due to their unconscious experience of clients’ holding onto them
as a form of voyeuristic intimacy, seduction, engulfment, or aggression (Langs,
1979). The apprehension therapists experience when a client asks them for more
time than they can afford to give may be due to their unstable marriage or
perhaps the erotic attraction they have to the client.
Dreams, Daydreams, and Fantasies
Dreams, daydreams, and fantasies are common means by which
the unconscious mind tries to get the conscious mind to help resolve
affiliative conflict. Thus, those which clients have during the course of
therapy often manifest TL, especially when their therapist
appears in them (Ferenczi, 1909). Similarly, those which therapists have often
manifest CTL (Tower, 1956), especially when their clients
appear in them.
Of course, sometimes figures appearing in dreams, daydreams,
and fantasies simply represent the person producing them. At other times,
however, they represent real-life persons with whom the dreamers, daydreamers,
or fantasizers have been in close and/or frequent conflictual contact.
Sometimes both are true, for the unconscious works hard to get the conscious
mind to help resolve conflicts. It counts on the phenomena it creates to get
through the barrier between it and its conscious counterpart.
Evidence-based methods of working with dreams, daydreams,
and fantasies, particularly dialoguing with dream figures, have proven
extremely helpful in understanding the nature of affiliative conflicts as well
as in finding effective ways to resolve them. Unfortunately, exploring these
methods is beyond the scope of this course.
Body Language, Complex Movement, and Somatization
Other well-documented manifestations of TL
are body language or simple movement, complex movement, and somatization. They
are universal, transcultural means by which the unconscious mind of one person
speaks to its conscious mind as well as to the unconscious mind of another
person through the body. Indeed, “the basic units of experience are [not words
but] bodily interactions between self and others” (Fast, 1992, p. 449). The bodily
action of both clients and therapists contains key information about what they
are trying to convey to each other (Scaer, 2005). Details of posture, gaze,
changes in skin color, and even respiration are noticed and unconsciously
recorded by both therapy participants (Meares, 2005).
Moreover, because the body cannot lie, it
is the richest, most accurate source of truth about what is going on in the
present and what aspects of the past have been embodied in memories. The body
has an uncanny “ability to tune in to the psyche; to listen to its subtle
voice, hear its silent music and search into its darkness of meaning” (Mathew,
1998, p. 185). It has the ability to do so, and seemingly cannot resist doing so.
Arguably, what happens on a one-time basis may not be worthy
of much attention. But body language that persists or repeats itself is. Again,
it is not possible to go into detailed explanations or skill-building here, but note
that facial indicators of unconscious communication are uniquely important.
Subtle movements around the left eye and left side of the mouth (Schore, 1994),
in particular, divulge hidden personalized feelings (Mandal & Ambady,
2004).
In contrast to body language that encodes a relatively
simple message, unintentional complex movement communicates several displaced
feelings and/or story-like thoughts. Thus complex movement that puts
transferred feelings and thoughts into action is termed enactment. Thoughts
and words become coercive action loaded with emotion that is related to figures
in the client’s and/or therapist’s past, including the very recent, minutes-old
past. It is action dictated by a “script” that is never actually seen, one
written by the unconscious.
Transferential enactments are a matter of clients
“assigning” to themselves and their therapist roles specific to past
conflictual experiences. Clients “intend” to play a part and have their
therapist play a corresponding one.
In the case of TL, clients unconsciously want
to have a wholesome affiliative experience with their therapist. Those clients still
conflicted over wanting to be nurtured gratis and not having
that experience with their biological parents might fail to bring their
copayments. Should therapists play a parental role by overlooking that breach
of contract, they may well be enacting their own countertransferential
conflict: needing to love unconditionally though they do not want to. Or
perhaps they feel compelled to make amends for damaging their own children by
not loving them unconditionally.
Similarly, therapists can enact their own
countertransferential affiliative conflicts by treating their clients as if
they were much younger than they actually are. For example, they might indulge
their clients by asking less of them than they are capable of doing. They might
absolve them of their obligation to change their behavior in a timely fashion.
They might continue to work with those who want to make their therapist a
friend well after they have attained their therapeutic goals.
Yet another manifestation of TL is
somatization: acting-in. A thought stimulates an emotion that finds
expression in a sensation. A thoughtless emotion, an unknown known (Bollas,
1987), expresses itself, usually in a sensation but sometimes in an inability
to move.
Transferential somatization manifests itself in physical
symptoms or bodily pleasures that have no real physiological cause. Common
examples are sudden stabs of pain, tears, trembling, strange sensations in the
solar plexus, poor sleep, and sensitivity to noise. Others are tightness in the
chest, nausea, rising heat, cramps, barely perceptible odors or tastes, and, most
revealing in the case of TL, sexual arousal (Boyer, 1997).
Indeed, somatization is the body’s revelation of what
happened earlier in the mind and “heart.” Hence, it can be a rich source of
information because so many unresolved affiliative conflicts occurred during a
preverbal stage of development. For instance, therapists’ feeling of repeated
and heightened physiological excitement when meeting with a particular client –
even preparing for it – can indicate how much those therapists are
unintentionally trying to meet their own affiliative needs. By contrast,
getting a headache almost every time particular clients come can indicate how
much therapists resent the clients’ requests to meet their affiliative needs.
What To Do with Manifestations of TL
- What is the first step a therapist must take?
- What determines how intently they must do so?
- Why is affect-regulation such an important task when dealing with
TL and CTL?
- What mistakes might be avoided by self-monitoring?
By monitoring clients?
- Is there likely to be a relationship between consciously taking
in transferential material and unique ways of establishing a therapeutic
alliance?
- What must therapists permit in order to regress while they take
in transference?
- What is dangerous about allowing regression?
- In what ways can manifestations of TL be decoded?
- What is the relationship between decoding and hypothesizing?
- What criteria should be used to begin testing hypotheses?
- What options do therapists have when they decide to test a
particular hypothesis?
- What would make one option more appropriate than another?
- Are manifestations of TL evidence of
things going on during sessions? Or are they data regarding
what is going on?
If therapists suspect that a manifestation might be an
affiliative communication disguised in one or more of its subtle forms, they
need to evaluate that possibility. How intently they should do so depends on
several criteria.
One is repetition. A manifestation that is repeated, such as
a thought that becomes an obsession, is more likely than not to be data
deserving further attention.
Another criterion is intensity. A dream one cannot shake,
for example, is more likely than not to be a transferential communication. So are
emotions that are clearly overreactions. So is bodily comfort or discomfort
that takes so much of one’s attention that it is virtually impossible to attend
to what a client is saying. So is doing something for a particular client that
one does not do for other clients. Going overtime with a long-term client who
says she is in crisis and cannot deal with it herself, for example, may not
actually be justifiable. Rather, it may be a sign of TL and/or
CTL.
Yet another criterion is unexpectedness; things being said
or done “out of the blue.” Beginning to reach out to embrace a client, for
example, may be a manifestation of CTL.
A final criterion is complexity. A dream that repeats itself
and causes one’s body to be noticeably tense is very likely to be
countertransferential. So is extending the session for a client who comes late
on a regular basis and then going home with a headache.
Vignette:
The intern naturally wanted to make a positive
impression on her supervisor. She wanted to be seen as mature and experienced.
She really liked one of her clients, and the attraction seemed to be mutual. He
not only kept all his appointments but started to share details of his affairs.
They became more and more sexually explicit. Fearing to be seen as complicit in
what was happening, the intern told her therapist what her client was doing but not how she looked forward to her sessions with him.
Finally, however, it became too much for her. She
could not shake what happened in his sessions; she kept having to say “No” to
thoughts and images of what went on between them. She decided to be candid with
her supervisor.
She was. She revealed the whole picture.
To her great relief – as well as surprise – her
therapist was pleased. She complemented her on suspecting TL and
CTL because it could be used therapeutically. If she and
her client could deal with it in his sessions, he could finally heal from the
early sexual abuse he had experienced with a nanny and relate to women in
non-erotic ways.
The intern was eager to develop the skills she needed
to have in her present and future practice: those that would make her
proficient in using TL and CTL
beneficially. She set out to learn the challenging task and subtasks she needed
to perform, along with strengthening her self-monitoring skills.
Overview of Subtasks
“As a blind man might come
across a gem in a heap of garbage, in this way the Awakening Mind appears
within oneself” (Shantideva, 7th century, India).
In order to deal well with TL and
CTL, we need to slow down our mental activity. We must be
like the blind man examining in his slow, methodical way the contents of the
“garbage.” We need to slow down the fast pace of our conscious mind and give a
manifestation of transference sufficient time to reveal its information. We
need to process what we suspect is unconscious communication.
Effective processing of a manifestation involves four
distinct but interwoven subtasks whose performance is a matter of supplementing
the logic of the brain’s verbal left hemisphere with the intuition of the
brain’s non-verbal right hemisphere. This is because TL, like
most relational transactions, relies heavily on speaker-listener cueing and
responding that occur too rapidly for simultaneous verbal exchanges and
conscious reflection (Lyons-Ruth, 2000).
In order to integrate bi-hemispheric communication
effectively, therapists must monitor themselves. They must evaluate how well they
are performing each subtask and decide when they should move from one to
another; whether to backtrack or move forward. In other words, therapists must
perform the subtasks separately as well as blend them into one multitask
process. So too must therapists monitor their clients in order to make sure
that they stay within a window of anxiety that permits meaningful work to be
accomplished.
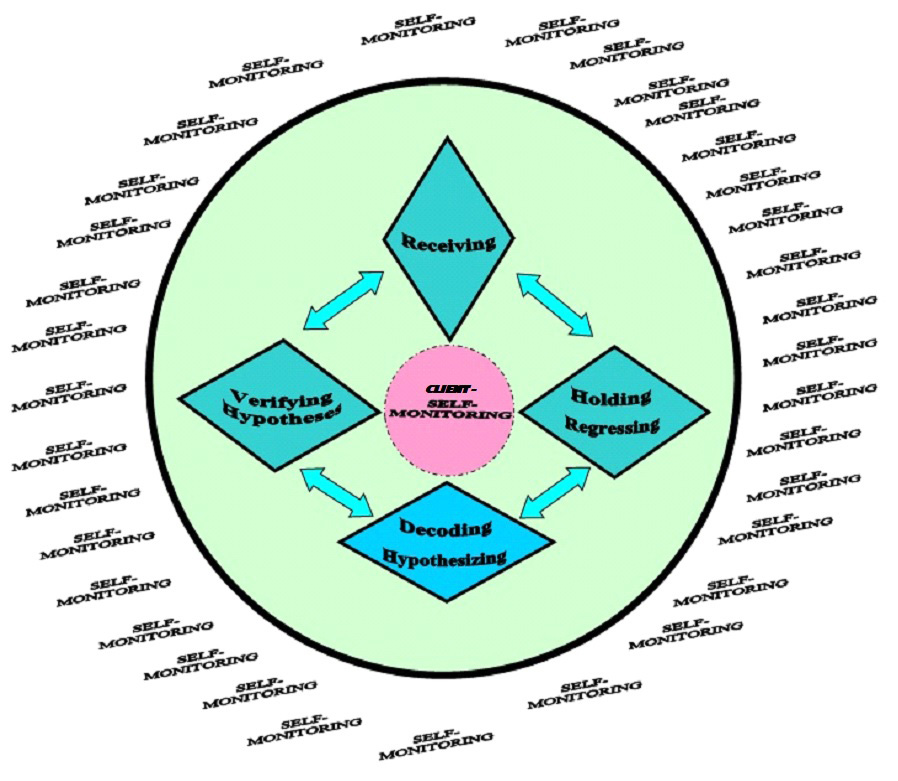
First Subtask: Taking-In Transferred Material
The first subtask is to take in consciously the
manifestations of transference we suspect we have already registered on an
unconscious level. This subtask requires us to deliberately open ourselves up
to what appears to be happening: conflict-laden contents in our clients’ and
our own unconscious minds are causing sensations and movements in our body
and/or thoughts, images, attitudes, and feelings that disturb us or make us
uncomfortable. But we really do not know why.
The first subtask is to “be there” for ourselves and our
clients in a new way (Heath, 1991). It is a matter of forming a composite
picture of conscious and unconscious information from which we can, in time,
derive fuller meaning than that based solely on conscious communication.
When we perform the first subtask, we intentionally “make room”
in our conscious mind for unconsciously displaced material. We choose to
increase our awareness of what our clients are transferring to us, and we are
consequently responding to it (Bird, 1922), along with what we ourselves are
transferring. We deliberately welcome past experiences that are replaying in
the present. We intentionally offer to our clients our “entire availability”:
all the time and mental space they need to deal with the unresolved conflicts
they are transferring to us (Grinberg, 1997).
In the course of increasing our awareness of clients’
TL, we are also bringing to consciousness our own
CTL. We are taking note of the roles we are unconsciously
assigning our clients and ourselves. If we are assigned the role of being a
parental figure for someone working through an early child-parent conflict, for
example, we deliberately “accept” a fleeting image of ourselves as an unloving,
self-indulgent person. If we are assigning the role of a disobedient, unlovable
child to our client, we hold in focus the self-righteousness we have begun to
experience from refusing to love that child. We allow ourselves to note, for
instance, the muscle tightness of one who is “teaching a child a lesson.”
In sum, the first subtask is a matter of combining how we
say, and/or how our clients say what they say, with what we or
they say. Furthermore, it is a matter of adding our own unconscious perceptions
and desires to the conceptions and intentions of which we are conscious. Put in
21st century neuroscientific and cognitive terms, we allow
right-brain learning to augment left-brain learning. We open ourselves to
receive nonverbal communication that cannot be put into words. Metaphorically,
we allow ourselves “to keep adding spices and seasonings to the soup we are
preparing, tasting frequently and adding one ingredient after another to bring
out the soup’s full flavor.”
Second Subtask: Holding and Permitting Regression
The second subtask is to hold the manifestations of
TL and CTL and to permit whatever
psychological regression happens in a deepened and broadened holding
environment. The second subtask is necessary because TL can be
safely dealt with only if it is fully experienced.
Thus, the second subtask is a matter of deliberately
embracing the full impact of our client’s unconscious communication. As we
continue to hold a manifestation of TL, we will come to realize
that “this is the clearer, sharper, more complete message my client is giving
me” (Smith, 2000). We make it possible for us to know experientially, for
instance, that “This client is both fearful of losing my love and angry with me
for not extending our session.”
We perform the second subtask by containing and
autoregulating our own negative states so that we can act as affect regulators
for our clients (Schore, 2003b). They can then experience us managing the
distressful feelings, sensations, and thoughts they have transferred to us.
They can continue to reveal their unresolved conflicts because we have not been
overwhelmed by the heightened anxiety that has kept those conflicts in their
unconscious mind. We are not only sharing their intrapsychic burden, but also
managing it.
As we do this, that burden already seems to be lighter to
the client. The safe holding environment provided by a therapist is one of the
most potentially healing vehicles a client will ever find (Wilkinson, 2003).
We must engage in affection regulation in order to perform
the second subtask (Casement, 1991). We must refuse to follow our natural
inclination to disengage from distressful communication. We must avoid closure
and tolerate ambiguity and uncertainty. We must choose to not understand
– for the time being – complex, displaced relational experiences (Schore,
2003a). We must not return to clients prematurely what they have put on us or
into us (Joseph, 1987).
The second subtask requires us to refrain from taking refuge
in words. We must resist the impulse to shift into a left hemispheric state of
mind and thus not respond verbally to transferred communication. Instead, we
must hold uncomfortable sensations and awareness evoked by that communication
(Stark, 1994). We must sustain the countertransferential feelings triggered by
the transference. We must stay in the right hemisphere’s processing mode, its
“Wait and See” (Federmeier & Kutas, 2002). We must do for clients what
they were unable to do for themselves during their original affiliative
experiences: allow psychic pain to remain in their conscious mind long enough
to be understood and processed.
Performed well, the second subtask typically results in our
having a somato-sensory experience of our clients’ unresolved affiliative
conflicts (Kernberg, 1987). We feel their anger, fear,
heightened sexual desires, and other distressful states. Thus we give them a
profound gift; we let them use projection and projective identification to
transform us into someone “bad,” someone deserving of disrespect, even abuse
(Gorney, 1979). We, not they, are now “bad.” They can experience relief. They
can be hopeful.
The second subtask also requires us to contain our own
unresolved affiliative conflicts; to re-experience the breadth and depth of our
own pain (Kernberg, 1975). We suffer the personal, painful
countertransferential feelings and sensations that we might well be projecting
onto or into our clients and thus triggering, or at least adding to, their pain
(Roth, 2001).
Needless to say, the second subtask is extremely difficult.
As we perform it, we are likely to experience excruciating emotional pain;
being found inferior, flawed, and valueless (Slochower, 1999), and thus
unlovable or unable to love. We are likely to regress to the point of
re-experiencing the rejection and humiliation that make early affiliative
experiences too painful to bring to conscious awareness. As our painful
emotional state exacerbates that of our client, we might even slip into a
psychologically primitive space. As our clients’ toxic material mobilizes our
own (Dosamantes, 1992) and we “return the favor,” we might even experience
quasi-insanity.
Quasi-insanity must not be underestimated. It is an
experience of disequilibrium within the right hemisphere. It easily leads to
deterioration in technical competence (Spence, et al., 1996) along with an
inability to think clearly and find appropriate words to use. It triggers
overwhelming fear of “losing it.”
Even so, the second subtask asks this of us. We must prepare
to deal with the unregulated or under-regulated forces that underlie
TL and CTL. We must temporarily relinquish
the adaptive goals and values inherent in our rational mind (Schwaber, 1990).
We must hold pieces of internal, unconscious phenomena that are not only
contradictory but also “crazy” and exceedingly disturbing (Isakower, 1963).
That’s the bad news.
The good news is twofold. First, regression can be managed.
It is not an all-or-nothing phenomenon that cannot be brought under control. We
can set limits to how long and to what degree we engage in it. We can end it
before it impairs our basic ego functions (Levin, 1997). We can come in and out
of it so that we never lose sight of the fact that what clients are
transferring to us still belongs to them (Deutsch, 1926).
Furthermore, we can stop ourselves from actually performing the transferential
roles we are being assigned or the countertransferential roles we are assigning
ourselves.
We can accomplish all of this by skillfully setting limits
to regression. We can interweave regression with grounding. We can make sure we
go back and forth between the then-and-there and the here-and-now. We can make
sure we dialogue with ourselves about what is occurring and what needs to be
done with it (Kernberg, 1987).
Second, regression gives us insight into what is actually
going on in the therapeutic interaction at hand and thus what is very likely to
be going on in extra-therapeutic interactions. As a consequence, it sheds light
on the affiliative conflicts a particular client needs to resolve. It enables
us to zero in on precisely what will ensure a positive therapeutic outcome.
Third Subtask: Decoding and Hypothesizing
Once holding TL and permitting regression
have yielded their fruits, we can decode or “break the code”: derive hidden
significance from apparent meaning. Thus we can bring greater clarity to what
we and our clients are trying to communicate about their unmet affiliative
desires and needs.
Decoding what our clients transfer to us is difficult
because we are simultaneously reacting to our own feelings, attitudes, and
thoughts. It is laborious because “transference [love] … has to be detected
almost without assistance and with only the slightest clues” (Freud, 1905,
p. 116).
Decoding is even harder with CTL. We
are “never in a favorable position to make a clear or clean-cut interpretation
of … countertransference” (Hedges, 1992, p. 22). We are extremely challenged in
decoding it as it is unfolding (Bennett, 2021). Hence, we must permit the third
subtask to be a multi-step process of interweaving intensive cognitive work and
meticulous attention to detail with the emotional-sensory-motor experiences we
are having.
First, we must identify what makes us suspicious. Is it the
client’s choice of words? Reported dreams or fantasies? Small movements? Or our
own tension? Then we must put to the side the apparent meaning of what we have
observed so that we can identify less obvious meaning, such as tone of voice,
volume, gestures that match or fail to match content, muscle movement that
supports or contradicts speech, and other nonverbal forms of human
communication.
We must also identify our own spontaneous response to what
we are noting: our feelings, sensations, thoughts, movements, and urges to do
something. We must determine whether they contradict or correspond to what our
client is overtly communicating. Those which contradict are more likely to be
transferential. Those which correspond may or may not be transferential.
Especially if they are exaggerated and/or sustained and/or repetitive, they may
be triggering our own unresolved issues.
Keep in mind, of course, that we are always
contributing something to our client’s transferential
communication. It is a matter of how much and to what degree.
Vignette:
“Why does this woman irritate me so?” the therapist
queried. “Why am I not simply flattered that she has asked to meet with me more
often? She is intelligent and articulate and seems to want to make progress.”
“Yet there seems to be something subtly seductive
about her. Though she does so nonchalantly, she keeps placing her hand on her
low-cut blouse.”
In looking at his own countertransference, however,
the therapist recognized that he was also experiencing distress in his abdomen.
He had to admit that he was frequently looking at where that hand was guiding
him.
“Something is not right here,” the therapist
acknowledged. “Although what I am doing corresponds to what she is doing – it’s
just a natural human response – I must get at the deeper meaning of what is
going on. What are some hypotheses?”
Hypothesizing, the second function of the third subtask is
a matter of determining possible explanations for why the phenomena we have
decoded are occurring; the most probable reasons why something that occurred in
the past has become part of the present. It is a matter of coming up with
possible causes of our clients’ and our own distress.
Ideally, hypotheses are simple statements. One hypothesis
about what is occurring in the previous vignette, for example, might be “I
am bringing to the sessions my own need for erotic love.” Or “I am
distressed because I should not have indicated that I am available.” Or “My client and I might both be contributing to my distress because both
of us have a need to love and be loved.”
Fourth Subtask: Verifying the Most Likely Hypotheses
The fourth subtask is a matter of verifying the most likely
hypothesis or hypotheses that we have formulated. Sometimes we simply do so by
ourselves. At other times we seek out third parties. At still other times we
share the hypotheses with our clients and ask for their feedback.
One would presume that the fourth subtask is easier than the
previous three, that just as we are eager to confirm our hypotheses, we are
also eager to disconfirm them. However, disconfirmation is more difficult for
us than confirmation, for formulating hypotheses inaugurates a fondness for
what we have conjectured and an unconscious search for supportive evidence.
Indeed, most of us do not actually want to re-consider our hypotheses. We just
want to accumulate more evidence to prove them – and ourselves – right. Hence,
the fourth subtask requires us to impose on ourselves the discipline of being
as objective as possible about our hypotheses and about whether we should
verify them by ourselves or do so with others.
When we have more than one most likely hypothesis, one
effective way to start is by paying close attention to our own somatic response
to the one that is most emotionally powerful. Our body will invariably, though
sometimes subtly, agree or disagree with what our mind is concluding. Being
physically energized, for example, usually suggests an accurate hypothesis,
while experiencing uneasiness or tension suggests the hypothesis is at least
partially inaccurate.
Third parties are invaluable during the verification
process. Particularly in cases involving significant CTL,
we would be unwise not to share our hypotheses with colleagues, consultants, or
our own therapist.
We might also share our hypotheses with our clients – sometimes
before, sometimes after consulting or meeting with our own therapist. If we
share sensitively and tactfully, we can give our clients a wholesome
interpersonal experience. They can learn how to clarify their affiliative needs
and desires and decide how best to pursue them rather than simply repeat
unsuccessful solutions or try an unpromising new one.
However, before considering just how we might share our
hypotheses with clients, let us explore a meta-task that must be performed
throughout the four subprocesses: monitoring.
Overarching Meta-Task: Monitoring
In order to use TL and countertransference
love benevolently, we must monitor ourselves to evaluate how well we are
performing the subtasks and auto-regulating our countertransferential love.
Concurrently, we must monitor our clients in order to make sure that they stay
within a window of anxiety that permits meaningful, even deep, experiencing of
transference, but does not overwhelm or retraumatize them.
We must maintain a “binocular vision” (Holmes, 1992). As we
attend to conscious communication, we must attend to our own and
our clients’ emotional and physiological functioning in the course of allowing
our unconscious minds to penetrate our conscious minds.
Self-monitoring begins with noting how well we are observing
our own CTL, for we must base our outward response to
clients no less on how they are doing than on how their displaced material is
affecting us. Clients may be extremely embarrassed, for example, and therefore
unable to hear what we have to say. At the same time, we may have become defensive
and desirous of setting limits to our clients’ expression of affiliative needs.
The question, of course, is always what is best for clients within the limits
of our own tolerance.
We must continuously self-monitor because TL
and CTL can impact the therapeutic relationship at any
time. We never want to either minimize or maximize them, but neither do we want
them to impair our clinical functioning. We want to give them enough “room” to
display themselves – even to develop – but not so much “room” that we end up
thinking poorly or acting unprofessionally.
As we self-monitor, of course, we monitor our clients’
tolerance levels. We observe how well they are auto-regulating by balancing
thinking with emotions; balancing judging; and wondering about, observing, and
controlling intrapsychic and intrapersonal phenomena. This monitoring allows us
to create the conditions under which clients can become increasingly aware of
what once was – and remains – conflictual, but not to repeat past
experience. Rather than have one more negative affiliative experience, they
should feel safe enough to risk feeling unsafe again in order
to work through their affiliative conflicts.
If clients assign us the role of a sexually abusive
caregiver, for example, we want to experience being one to the degree that we
realize what our clients have gone through. Concurrently, we want clients to
realize that we know experientially what they have gone through. However, we
are not going to go so far as to abuse them, even verbally. Rather, we are
going to help them learn how to defend themselves from being victimized in the
present, and to lower, if not erase, the power victimization memories have over
them.
Similarly, if clients displace positive feelings toward us,
such as experiencing us as a nurturing mother figure, we will allow the
TL to continue until basic bonding takes place. But we will not
allow clients to become dependent on us to meet their need to be nurtured. We
will not console them each time they are disappointed or protect them from
feeling abandoned when we go on vacation. We will not be the mother figure they
are capable of being for themselves.
Monitoring is important during the first subtask when we
consciously take in TL and CTL
(Hinshelwood, 1999), for we need to decide whether we might perform those roles on
a temporary basis as a means of bonding with clients. Those who feel
very unlovable, for example, might benefit from time-limited signs of parental
acceptance and approval. They might not be able to bond with those who do not
appear to accept or approve of them. Even so, they need to learn to accept and
approve themselves along with experiencing maternal and/or paternal
love from appropriate people in their everyday lives.
Monitoring during the first subtask also enables us to gauge
the extent to which we are unconsciously projecting our own unresolved
affiliative conflicts onto or into our clients. Without this internal
supervision, even experienced therapists are prone to simply re-enact their own
and their clients’ maladaptive interpersonal experiences in
countertransferential behaviors (Dreher, et al., 2001). As a result, clients
and therapists never realize the contributions they make to therapeutic
failures, nor determine how they might conduct themselves differently (Weiss
& Sampson, 1986).
Monitoring is crucial during the second subtask when we
contain transferred material and permit regression. We must stay with clients
on a psychobiological level in order to engage in necessary experiential
learning. But we must not go so far as to lose our ability to stand apart and
take note of our participation in the realms of TL and
CTL (Racker, 1968; Gorkin, 1997; Gelso & Hayes, 1998; Nissen, et al., 2020).
We must remain disengaged enough to ask questions such as “Is my client trying
to seduce me?” and/or “Am I being seductive?”
Monitoring becomes especially important when we permit
conscious regression. We must become vulnerable to the workings of displaced
material at a sufficiently – but not dangerously – deep level (Winnicott,
1965). We must be partially aware of the process we are undergoing in order to
discontinue it at any time. We must periodically employ our observing ego to
“keep track of the pressure to become trackless” (Schafer, 1977). We must
“swim” in the sea of others’ TL but not “drown” in our own
CTL” (Racker, 1968, p. 16).
Furthermore, only if we monitor our own regression can we be
aware of the regression our clients might be undergoing. They can benefit only
from carefully regulated exposure to the pain that so overwhelmed them in the
past that it could not be processed. They cannot benefit if they are re-traumatized.
Monitoring is necessary during the third subtask when we
decode and hypothesize about TL, for it is operating even as we
are deriving meaning from it, and determine exactly what is going on. We must
stand aside to decode and hypothesize yet remain available to our clients. We
must not allow the length and intensity of the decoding and hypothesizing
processes to do away with interpersonal contact. Clients want to be accepted,
listened to intently, and followed closely. We harm them if we engage in
difficult cognitive tasks for what seems to them to be “forever.”
On the other hand, we need to self-monitor to see if we are
allowing ourselves enough time to decode and hypothesize. Though we may not be
certain of what is occurring, we must come up with hypotheses that can be
tested.
Monitoring is crucial during the fourth subtask when we verify
hypotheses, for we need to balance testing hypotheses with keeping an emotional
connection with our clients. At the same time, we must continue to receive and
hold new material that will allow us to revise inaccurate hypotheses.
Finally, we must monitor during all four subtasks in order
to be able to move quickly and smoothly from one subtask to another. At times,
we must decode what we have uncovered in order to know what more we need to
discover. Similarly, we may need to experience more in order to verify what we
think we understand. At other times, we must gather new information in light of
our hypotheses proving inaccurate. At still other times, when we suspect
inaccuracy, we must stop decoding and test our hypotheses. Put simply,
wholesome interpersonal interactions rely heavily on monitoring our decisions
related to focusing: what to focus on, whom to focus on, where to focus, and
even how to focus (Hubble, 1999).
To summarize, by systematically performing the four subtasks
while judiciously monitoring ourselves and our clients, we can know our clients
on a deeper, more meaningful level than we could otherwise. We can also gain
insight into ourselves. Thus we can facilitate a detoxification process whereby
clients can finally address their unconscious affiliative conflicts. They can
strip transferential material of its dangerous characteristics (Grinberg, 1997)
and use the truths it reveals to finally meet their affiliative needs.
How, Why, and When to Engage Clients in Hypothesis-Testing
- With what attitude should therapists engage clients in
hypothesis-testing?
- What might make it hard for therapists to test hypotheses with
clients?
- What are the benefits of inviting clients to evaluate the
accuracy of hypotheses?
- What exactly are transference interpretations (TRIs)? Countertransference interpretations (CTRIs)?
- What makes TRIs and CTRIs similar? Different?
- What criteria do TRIs and CTRIs meet when they are effective?
- Why should TRIs and CTRIs be used selectively?
- Why should TRIs and CTRIs be timed carefully?
- Why should TRIs be used infrequently and combined with other interventions?
- With what kinds of TL are CTRIs usually essential?
- What are some major problems that might result from not using
TRIs and CTRIs?
Attitude Required of Therapists
Therapists who share their hypotheses about TL
and CTL provide a protective factor for both themselves
and their clients by fostering within themselves an attitude of humility and
detachment. They thereby reveal that they do not have all the
answers. They are simply observing and wondering. They are saying to their
clients, “Let us together determine whether what I think is going on between us
rings true for you. I can – and want to – learn from you” (Churchill, 2019).
To observe and wonder with humility and detachment is not to
have an agenda for what clients are supposed to think or feel. It is not to
be ahead of clients in ascertaining personal and interpersonal reality. Indeed,
it is to be open to whatever happens when two persons try to understand
unfamiliar phenomena. “As clinicians, we are enjoined to be agenda-free; we may
have our preferred models of the mind, but they are not to be superimposed on
[clients’] material” (Schwaber, 1990, p. 237). We are to simply observe and wonder
so that we do not become attached to our interpretations, despite our attempts
to treat them as hypotheses (Cooper, 1993).
To simply observe and wonder rests on therapists’
willingness to describe nonjudgmentally what seems to be TL and
CTL. Particularly in non-analytic therapy, an effective
interpretation of both TL and CTL rests on
an attitude of “I know less rather than more” (Schwaber, 1990). It echoes what
Winnicott (1960) said whimsically: “I interpret mainly to let the [client] know
the limits of my understanding” (p. 711).
In other words, therapists need to be open to rejection or
revision no less than acceptance or confirmation of their hypotheses. They need
to respect clients’ experience of their therapy sessions and their relationship
with their therapist.
At the same time, therapists need to bring directness,
pertinence, inclusivity, and concreteness to what are fundamentally subjective
experiences. Rather than dispense truths and meanings, they prepare for a
trial-and-error process involving dialogue with their clients (Cooper, 1993).
They need to await something relatively definitive: truth that requires the
active cooperation of clients to develop (Bezoari, et al., 1994). Indeed, both therapists
and clients are holders of partial truths that can be known in their fullness
only when the parts are shared. Indeed, if TL or
CTL are occurring during therapy, it will be verified –
eventually, if not at the moment – in the psyches of both therapist
and client.
Therapists who wish to collaborate with their clients to
verify suspected TL and CTL begin the
process by using a transference or countertransference interpretation.
A Transference Interpretation
A transference interpretation (TRI) is an explicit reference
to what a client appears to have displaced from the past, including the very
recent past, to the present therapeutic setting. A TRI makes unconscious
material conscious so that it can be subjected to legitimate evaluation. If it
is inaccurate, it can be revised. If it is accurate, it can be used to resolve
an intrapsychic affiliative conflict.
A TRI is “a creative re-description that implicitly has the
structure of a simile. It says, ‘This is like that’” (Schafer, 1977, p. 57). A TRI
reveals how present behavior is a re-enactment of past experience rather than
something happening on its own. “I wonder if I strike you as maternal when I
keep listening to you even though our time is up,” is a TRI related to an
affiliative issue.
The use of TRIs is based on a therapeutic premise espoused
by clinicians of major theoretical orientations; it is crucial that TRIs be
subjected to legitimate conscious evaluation as well as to unconscious
attitudes and beliefs to which clients have been holding fast. Some of them may
be adaptive and thus worth holding. Others, however, may have been adaptive in
the past but are detrimental to wholesome relationships in the present. They
create unresolved conflict-based anxiety both for the one who holds them and
for the one to which they are supposed to apply. “I don’t care if my father
does not love me because my mother does,” a client may have believed as a
child. That belief – that maternal love can replace paternal love – kept anxiety
in check at the time. Thus it became a schema or principle of knowing that the
client could unconsciously use in both male and female relationships. It became
a “certainty” in spite of its never being validated (Schafer, 1977). As a
consequence, a client who holds the schema continues to rely only on maternal
love without questioning her belief. She not only overvalues it but also
requires one maternal figure after another to play a maternal role in her life,
even though having to mother another adult does not work well for most maternal
figures. Even if it did, because the client is no longer a child, it is
developmentally inappropriate. Hence, it is “ripe” for processing by means of a
TRI.
In brief, a TRI is intended to help clients acquire new
experiences from which more adaptive principles of knowing can be derived and
reality-based schema can be created. The TRI above, for example, is intended to
help the client question her belief that all maternal figures should be willing
to give her extra time and attention because she must rely
primarily on maternal love. It is intended to help her restructure an old
belief and resolve its underlying conflict: being an adult biologically and
intellectually, but a child emotionally and interpersonally.
A TRI is a therapist’s means of asking clients to consider
how their thoughts and feelings toward their therapist might be coming
primarily, though not solely, from past experiences with persons similar to the
therapist. “Could it be that your resentment toward me because I ended our
session on time is tied to your mother’s not giving you enough attention?” a
therapist might ask.
Though it may or may not directly mention the client’s past,
a TRI is intended to address what the client has displaced from the past.
“Could it be that you are sad because I kept you waiting, as did your mother?”
and “Could it be that you are sad because I made you wait?” are both acceptable
TRIs. So are “Could it be that you are frustrated with me because I reminded
you of your unpaid fee the way your teachers reminded you of unfinished
homework?” and “I wonder if your sadness comes from my telling you that I will
be on vacation for two weeks.”
Thus a TRI is an invitation for a client and a therapist to
consider together various explanations for the dynamics of their sessions, to
tease out what is past-based or outside-of-therapy-based and what is actually
happening in their sessions. It is an invitation to distinguish between the
past and the present, as well as between the in-here and out-there foundations
of feelings and thoughts. A TRI is an implicit acknowledgment of the powerful
impact that people not actually in the therapy room – and events connected with
them – can have on what arises in therapy. A TRI is also an implicit
acknowledgment of the need to make conscious an unconsciously held maladaptive
attitude or belief.
Though a TRI may be stated in the declarative as in “I think
you may be sad because I acted like your mother,” it remains open to
evaluation. Thus, “When the interpretive process is working well, therapist and
patient are engaged in the exploration of hypotheses [regarding their
relationship] arrived at by a collaborative process” (Meissner, 1996, p. 257).
Vignette:
At the beginning of the session, the therapist
remarked that her client had not paid her fee for the third time in a row.
Though the client acknowledged this and promised to send a check the following
day, she responded curtly to several of her therapist’s subsequent compliments
on her accomplishments that week. Recalling the client’s accounts of her overly
critical father, the therapist finally said, “It seems to me that you are
annoyed with me today, perhaps because by referring to your unpaid fee I
reminded you of your critical father.”
Using this feedback, the client admitted that she
was angry with her therapist. She refused to admit, however, that she was
expressing that anger inappropriately.
Two sessions later, though, when the therapist again
made a tentative connection between the client’s brusque dismissal of her
therapist’s observations and her father’s criticism of her, she conceded. She
was then able to slowly own the painful humiliation she still experienced when
others found her at fault. Thus, TRIs enabled client and therapist to explore
previously inaccessible material.
A Countertransference Interpretation
A countertransference interpretation (CTRI) is an explicit
reference to the client-therapist relationship as
the therapist is experiencing it. “I wonder if I am hurt by your continued silence today, just as
you were when your mother ‘cold-shouldered’ you,” is an affiliative-related
CTRI.
CTRIs are based on therapists’ countertransference: what a
client has displaced onto or into them, or what therapists transfer to a client
from their own past. Thus, CTRIs reflect the fact that countertransference,
like transference, is co-created.
Said a little differently, CTRIs are revelations of
therapists’ reactions to what a client does and/or says. They are means of
sharing what therapists believe a client is unconsciously communicating as he
or she is reminded of past events and persons. They are also means of sharing
what therapists are bringing from their own past to the
therapeutic setting. “I am hurt by what you just said. I wonder whether that
reminds me of how my mother hurt me,” a therapist might say when describing
both transferential and countertransferential love phenomena. Another example
would be, “Could it be that my headache is due to how hard it feels to have my
thoughts accepted by you today?”
It might appear as if CTRIs are invitations to explore therapists’ conflicts.
But that is not the case. Rather, CTRIs are ways into exploring clients’ conflicts.
To make that clear, therapists might need to add to a CTRI something like,
“You, not I, are our focus, even though I told you that I am attracted to you.
How do you feel right now?” (Danzer, 2018).
Ideally, CTRIs refer to a conflict that therapists are
experiencing while working with a client because that conflict is likely to
have been identified, or at least implied, in the client’s presenting problems.
Consider, for example, this CTRI shared with a client wanting to deal with her
habit of obsessing about the mistreatment she has suffered:
“When you focus repeatedly on how badly you were treated, I
begin to feel mistreated myself. I feel trapped in an unending hopeless
situation.”
Vignette:
The client elaborated on a pleasure trip he had just
made, providing comical anecdotes interspersed with interesting descriptions.
Though at first the therapist was intrigued by her client’s account, she soon
noticed herself becoming morose. The incongruity between his enthusiasm and her
negative response was striking.
The therapist began to recall confronting her client
previously about taking numerous trips with his friends in light of his goal
being to spend more time with his autistic son. She also believed that she had
modeled how to put the child first by rescheduling an appointment so that the client
could attend his son’s school play.
Suspecting TL, the therapist
interrupted her client and said, “I’m saddened by your account of your trip. Is
it shedding a light on how your son might have felt when you left home without
him?” Then after pausing, she added, “Could it be that my sadness is what you
also feel when you focus on your child?”
Thus the therapist suggested what might be at the
heart of her client’s difficulty in implementing his goal: the deep sadness
that impairs his judgment when it comes to choosing himself and his friends
over his son. Though it was true that the therapist was also recalling times
when her alcoholic father’s failure to keep his promise to come to her school
events caused her deep emotional pain, she did not refer to it in her CTRI.
Rather, she chose to set an appointment with her own therapist.
In sum, CTRIs are intended to shed light on the heart of the
matter, the reason for clients’ presenting problems: why they might find it
challenging to bond with another, for example, in spite of their good
intentions; what they might need to address before they can
even address their goals as such; and how they might be
contributing to problems they see as being caused solely by others. If
countertransference truly opens the “door to a slice of life,” a CTRI holds
that door open. It enables therapists and clients to collaborate in observing
and exploring what they may never have suspected. Then, when new insight and
emotional processing follow, the “slice of life” has yielded its rich contents.
Vignette:
The client insisted that his wife, who had
recently divorced him, was unjustified in saying that she was doing so because
of how angry he was. He was conscious of the opposite: he did not express his
anger, he simply accepted her verbal abuse and went on. “As long as she takes
good care of the children,” he told himself, “I can live with what she does to
me. I do not have to retaliate or even express my own anger toward her.”
However, gradually his therapist became aware of
subtle signs of feeling belittled during sessions. It seemed that he routinely
corrected her reflective summaries with low-grade impatience and subtle
criticism. His facial expression and tone of voice said in effect, “You didn’t
remember what I told you and therefore missed the mark again. You should be
smart enough to remember and get it right!”
She reminded herself, however, that she saw him at
the end of a long day. “It is annoying to hear distortions of what you say,”
she added to his criticism. “I might need to change the time of his
appointment.”
But she also heard the nagging thought: “I am not
an acceptable person because I do not remember all the details my client shares
with me. I am not that perfect recorder of his communications, that infallible
computer that encodes every communication given me.”
Rather than change his appointment time, she chose
to stay with the pain of being an unacceptable person. It reminded her of how
she had been found unacceptable by her best friend in middle school and her
mother’s dismissal of it as just “an opportunity to get rid of a ‘bad apple’ by
finding a really ‘good apple.’”
As she purposefully regressed in performing the
second subtask, the therapist experienced excruciating sadness related to her
own past. She also noted subtle signs of distress in her client: his fighting
back tears, his furrowed brow, and his hunched shoulders. “Could it be,” she
asked herself, “that he tried hard not to express his anger toward his wife in
the hope of at least keeping her at least nominally in their marriage? Was he
doing the best he could to prevent her from finding him unacceptable?”
Because her countertransferential reaction allowed
her to put her finger on what neither she nor her client had previously
suspected, she was able to hypothesize. “The indirect expression of his anger
might well be what his ex-wife had experienced: his passive-aggressive,
difficult-to-identify expression of anger.” This insight permitted her to
formulate a CTI: “I feel belittled when you correct what I say, even though I
believe you are not consciously demeaning me. Could your ex-wife have felt the
same way?”
Though her client wanted to dismiss the
interpretation as meaningless, he was willing to look at it when he sensed his
therapist’s empathy. In the next session, he entertained the thought of how
hurt his wife may have felt. In subsequent sessions, he made efforts to stop
himself in the course of correcting his therapist. He was on his way to
addressing what he had contributed to his marriage ending in divorce.
Interpreting countertransference is especially valuable,
perhaps even essential, when clients have experienced trauma at preverbal
stages of development or trauma so severe it could not be put into words. In
cases like these, it is only through countertransference that therapists can
gain insight into the troubled world of clients (Racker, 1968; Sandler, 1976;
Viederman, 1974), phenomena already “known” to them on some level (DeLaCour,
1985; Herron & Rouslin, 1982; Lear, 1993).
Vignette:
Regardless of how many times the therapist returned
her client’s frantic phone calls – or chose not to in non-emergency situations
– he consistently rebuked her for either taking too long or not doing so at all
when she sensed she was being manipulated. She found herself feeling resentful.
She became increasingly eager to enforce the limits she had set early in their
work: no phoning between sessions unless there was a true emergency. She could
put the matter on the table without damaging the therapeutic license, she
thought. “Though he was severely abused and neglected as a child, my consistent
patience and responsiveness over the three years of our work have certainly
given him ample evidence of my care and concern,” she reasoned.
So she endeavored once again to help her client see
how some of his frequent phone calls were not as necessary as he made them out
to be. Nonetheless, each time, the client disparaged his therapist’s viewpoint
and protested that he had to have his phone calls returned.
Finally, the therapist decided to share her
countertransference. She said in a calm voice, “I’m feeling resentful because
it seems as if your frequent phone calls are making me the parent to an adult.
Could we talk about this?” During what ensued, the therapist added that she
might have been trying too hard to be an all-good mother to make up for his
experiences of an all-bad mother. Then, when her client continued to have
difficulty appreciating his therapist’s feelings, she said, “When I feel
verbally abused for not being responsive to you, I feel like separating myself
from you, even at times of true emergencies.”
At the time that the therapist voiced the second CTRI, her client was incredulous
but willing to talk about what she said. During the following week, he called
only once. Shortly thereafter he playfully referred to her as “a mother that
had to have time for herself so that she could be there for her children when
they really needed her.” During his termination session, he described his
therapist as the "good-enough mother” he had never had as a child.
Thus, by using carefully worded CTRIs, the therapist
modeled how to be honest as well as how to explore unintended consequences of
her client’s behavior. She gave him a real-life example of how his behavior was
contributing to his unmet affiliative needs. Additionally, by interpreting her
countertransference, the therapist strengthened the therapeutic alliance. She
offered concrete and convincing evidence of her attunement to her client and
her willingness to accept and respect him. She gave him a safe place to
consider replacing his maladaptive way of meeting his nurturance needs with
more adaptive ones.
To summarize, TL-related TRIs and
CTL-related CTRIs are statements or questions that shed
light on client-therapist dynamics in therapy sessions related to affiliative
needs. They are means of bringing into consciousness unresolved conflicts
regarding those needs. They are invitations to identify distortions, misinterpretations,
and unfair attributions as a prerequisite for arriving at accurate meaning.
They enable clients to work with their therapist to replace old schemas and
patterns of relating with other people with new, age-appropriate ones. Thus
they give clients an opportunity to finally meet their affiliative needs,
perhaps not totally, but as satisfactorily as possible. That’s the good news.
The bad news is that TRIs and CTRIs regarding TL
and CTL are usually uncomfortable for therapists to voice
and for clients to hear. If they refer to negative phenomena, they can make
therapy participants experience embarrassment and shame, if not humiliating
rejection. If they refer to positive phenomena, as does “I find myself
attracted to you, partly because you are open about your sexuality,” they can
make a therapist appear seductive (Audet, 2011). Furthermore, if shared TRIs
and CTRIs are verified by clients, they call for the difficult, risk-taking
work of replacing familiar old patterns with unfamiliar new ones. Thus,
therapists tend to shy away from using them.
The good news is that if TRIs and CTRIs are worded carefully
and shared sensitively, they create a safe environment in which to launch that
hard work.
Vignette:
The client, a mid-ranking naval officer, kept coming
to therapy but made only minimal progress in managing her anxiety in spite of
learning and using several new cognitive-behavioral interventions to reduce her
anxiety during presentations she made to her superiors. If she couldn’t stop
having these near-panic attacks, she might well be demoted, she feared.
Very early in therapy, she had revealed her
extra-marital affairs to her therapist, but six months later she said that she
had not engaged in any inappropriate relationships since beginning therapy.
“Why then,” wondered her therapist, “did I get sexually stimulated during our
last session? She is clearly an attractive woman, but I greatly enjoy my
relationship with my wife. Why now? What might I be contributing?”
When his countertransferential reaction re-occurred
in the following session, he decided to use a CTR: “My sexual attraction to you
is getting to be a problem for me. Can we talk about what might be going on
between us?” His client seemed to freeze as she heard his words. She opened her
mouth slightly but could not speak. After some silence, however, she said that
she was seriously considering having an affair with a married colleague.
Nothing had happened yet, but she had been struggling for a few weeks.
With this disclosure, the therapist was able to help
her better understand why she continued to be anxious when meeting with her
superiors. The military would never condone what she was thinking of doing. Her
entertaining the idea of such an affair was an impediment to managing her
anxiety. She had to make a choice.
Qualities of Effective Transference Interpretations
Calming
TRIs (including CTRIs) are to be given in such a way that
they calm clients (Strachey, 1934). However clients respond, they will not be
criticized. They can deny, confirm, question, revise, or reject the TRI, all
with impunity.
TRIs calm a client when therapists simply indicate that they
have received a communication from their client. This holds even though it
might be a criticism (Casement, 1991). An example would be, “I wonder if by
coming late you are telling me that in the last session, I said something
hurtful. Am I right?”
Bollas suggests that therapists introduce TRIs with such
calming phrases as, “What occurs to me,” or “I have an idea,” (Bollas, 1987, p. 206)
or “I’m curious about what you think of this,” or “I’d like to share a thought
with you,” or “You may not agree with me but …,” or “I wonder.”
TRIs that calm clients make them feel secure. Their
therapist can survive the negative thoughts and feelings they have transferred.
Their therapist can hold their projections up to the light of scrutiny without
“falling apart” or being devastated if their negative messages are confirmed.
Of course, therapists must convey calm through such prosody
as tenor, volume, tone, and pitch. In some cases, they must even add a
respectful look and/or a reassuring gesture or facial movement.
In order to make TRIs calming, therapists might need to take
a moment between hearing and speaking; a short pause between what clients say
and what they say. During that time, they can address their
own diminished capacity to think clearly due to strong emotional reactions
(Churchill, 2019). By pausing, they give evidence of their “holding” their
client’s communication calmly before using gentle wording to asking them to
consider the truth it might reveal.
Emotionally Immediate
TRIs must also be emotionally immediate (Strachey, 1934; Nissen, et al., 2020).
They must clearly identify distressful or problematic emotions, however
uncomfortable it may be for both client and therapist to hear them.
Furthermore, to be most helpful, TRIs should be given as closely in time as
possible to clients’ experience of their feelings. An example would be “Could
we stop and explore what might be the need you have when you ask if we could
meet in a restaurant?”
At first it seems a contradiction for a TRI to be both
calming and emotionally immediate. But these qualities are not actually
mutually exclusive, because emotions can be expressed in varying shades of
intensity. The challenge for therapists is to find that balance between
accurate reflection of and containment of the client’s feelings. Even a TRI
like “You seem to hate me. If that is true, can we talk about it?” can be said
in a polite tone of voice. Thus it conveys that although hate seems to be the
primary feeling of the client toward the therapist, the therapist has not
internalized the hate. Moreover, it is not being returned.
With certain kinds of material, it is especially important
for therapists to make TRIs emotionally immediate. In the realm of sexual
abuse, for example, if a therapist waits too long to interpret a client’s
communication, the client may experience the therapist as being afraid to face
facts. As a consequence, the therapist’s activity can become a re-enactment of
a past person turning a blind eye to the client’s plight (Casement, 1991).
Neutral
TRIs must be neutral statements, not unquestionable
pronouncements or indisputable moral judgments. They must come across as
objective observations that expose, clarify, or explicate. They simply reflect
what the therapist has noticed.
TRIs should be voiced without defensiveness on the part of
the therapist (Gill, 1982) because clients “are acutely sensitive to the hidden
meaning in what their [therapist] says. It is harmful … when [therapists]
appear to ignore a client’s accurate perception or interpret defensively in the
face of it” (Casement, 1999, p. 131).
Neutral TRIs invite clients to observe what seems to
be the case; to check out their therapist’s impressions (Schwaber, 1990). They
are invitations to do some reality-testing in order to acquire insight
(Casement, 1991). They give clients the “okay” to feel and express feelings,
even very primitive ones (Gill, 1982), with impunity.
Neutral TRIs are devoid of moral judgments. They do not
suggest to clients that their therapist finds them guilty of something. Thus
therapists say, “You may be angry with me,” or “You appear to be angry with me,”
or “I believe you are angry with me,” rather than “You are angry with me.”
Of course, the requirement to keep TRIs neutral requires a
tolerant tone, restrained tenor, modulated volume and speed, subdued pitch, and
dispassionate inflection, all of which combine to create mood and interpersonal
atmosphere. TRIs voiced with neutrality enable clients to conclude that their
therapist is simply noticing. This is extremely important because clients tend
to listen primarily to “mood;” some do not even hear the words (Pick, 1997).
Especially when very disturbed and in need of soothing, clients acutely scan
interpretations to assess what is happening in their therapist’s mind
(Hinshelwood, 1999). Is it retaliation? Is it resentment? Is it forgiveness?
Examples of TRIs that connote neutrality are:
“You may be angry because …,”
“It appears as if you are angry because …,”
“I wonder if your anger with me is something even you don’t
feel good about,”
“I wonder if you are suffering a great deal from punishing
yourself,” and
“It’s almost as if you are experiencing this suffering as
some kind of punishment.”
An important corollary to making TRIs neutral is that it is
helpful for therapists to use what they think they know and to
find a way of approaching this through not yet knowing rather than to simply reflect what clients are saying. “You seem to be suffering a great
deal from punishing yourself,” and “It is almost as if you are experiencing this
suffering as some kind of punishment, but it isn’t clear what you are feeling
guilty about,” are examples of TRIs worded with the “not yet knowing” corollary
in mind. They convey that the therapist needs the client’s collaboration to
arrive at the truth of the matter.
When clients use strong terms in describing themselves or
others, formulating neutral TRIs becomes a special challenge. For example, soon
after a therapist has set limits to the client’s in-session behavior, an
adolescent might cry, “My mother is a witch!” To maintain neutrality and calm,
and yet keep the interpretation emotionally immediate, the therapist might
reply, “You put great emphasis on how your mother is a witch. Would you like to
say more about that?” An alternative might be, “I wonder if by referring to a
witch you are saying that you find your mother mean to you. Am I on target?”
Still another would be, “I wonder if you are referring to me when you say your
mother is a witch.”
In phrasing TRIs in these ways, therapists play back
clients’ descriptions as clearly the client’s perception,
rather than both the client’s and the therapist’s. Thus therapists keep a
balance between respecting clients’ points of view as subjectively valid and
questioning their objective validity; that is, not necessarily being objective
facts. As a consequence, the therapy room stays a safe and secure, open and
receptive space in which to process what is most disturbing to clients. Their
therapist has remained neutral but has also noted the forcefulness and
immediacy of their feelings. They can safely look at a painful experience that
they might or might not be perceiving accurately.
Neutrality is extremely important when clients give feedback
in such a way that therapists feel criticized. They must then find some way of
dealing with their clients’ experience without reacting with hurt feelings or
anger that would dissuade clients from being honest in the future.
At times it is best for therapists to simply refrain from
even naming their client’s or their own feelings. They can simply acknowledge
what is transpiring, as in “I can see how you could have heard what I said as
critical.” If, by contrast, therapists focus first and only on transference or
countertransference feelings, clients might experience their therapist as
defensive and intent on denying elements of objective reality in the client-therapist
relationship (Casement, 1991).
Precise, Clear, and Concrete
While TRIs are neutral, they must also be precise and clear
about the TL distortions clients seem to be making, or about the
specific relational actions that are affecting their therapist (Kiesler, 1982).
They are specific: detailed and concrete (Strachey, 1934).
TRIs are not abstractions or vague assertions. In all
likelihood, for example, clients would hear, “You seem to be getting upset
about what I’m saying,” as an ambiguous remark. They might also have a chance
to thwart their therapist’s attempts to make unpleasant unconscious material
conscious (Strachey, 1934). They might take the opportunity to slip out of responsibility
for their communications into what has felicitously been called a “gentleman’s
agreement.” “We won’t get into difficult, painful matters,” that unspoken
agreement goes. “We will just note in passing that we don’t feel comfortable
with something going on between us. Like gentlemen, we will cease and desist
and thus resume our comfortable relatedness” (Wolstein, 1996, p. 507).
If, on the other hand, TRIs clearly identify observable
signs or manifestations of the suspected transference, clients are given a
sound foundation on which to consider their therapist’s hypothesis. If the
hypothesis is shared in a clear, concrete, and precise TRI, and it is true, the
client will resonate with it. Intrapsychic boundaries will be permeated (Lear,
1993). Client and therapist can then collaborate to discover the exact nature
of an interpersonal affiliative issue.
“Could it be that you are angry with me because I said your
behavior is inappropriate?” is clear and concrete. So is “You seem to be
resentful because I commented on your tardiness.” So is “I’m wondering if you
dislike me now that I have questioned whether the blame is entirely your
sister’s.”
Tentative
Effective TRIs are tentative. They are not as
informative as communicative (Brodbeck, 1995), not as certain as
probabilistic (Schafer, 1983). “Could it be that…,” “I wonder if…,” and
“Perhaps it’s that…” all invite the client to respond in agreement,
disagreement, or partial agreement. Thus TRIs pave the way for further
clarification. They allow therapists to watch and listen for evidence of
consensual reality or organized experience that supports clients’ and their own
perceptions or conclusions (Schafer, 1983).
Tentative TRIs are intended “to be played with – kicked
around, mulled over, torn to pieces – rather than regarded as … official
versions of the truth” (Bollas, 1983, p. 7). If therapists come across as certain rather
than tentative, clients then have to contend with an individual who seems to
already know what is going on. They have already decided what the client is
contributing – versus what the therapist is contributing – to an interpersonal
problem in therapy. But the truth is that there are no reliable means of
identifying for sure what belongs to whom (Field, 1989) other than through
interactive work: client and therapist testing the validity of the TRI together
(Bacal, 1990).
Thus, clients benefit from TRIs that therapists phrase
tentatively. Far from being dogmatic and certain, therapists make it clear that
they are intending their perceptions to be explored for potentially different
meanings (Winnicott, 1971). They are offering to their clients “a scrap of
material and a chance to elaborate on it (Bollas, 1987, p. 206)”, a chance to
ponder rather than automatically validate feelings and judgments.
Tentative TRIs tend to convey that therapists are having
difficulty putting into words what they believe their client is feeling or
thinking. When therapists openly struggle to find the right words, they model
how to deal with what they somehow “know” but cannot easily describe or what
they suspect but do not really know. They counteract that certainty with which
clients have often been judged and judge themselves. They invite clients to
collaborate in an effort to discover the complexity of the human person,
especially in relationships. They emphasize the value of putting subjective
experience under scrutiny (Bollas, 1987).
Pertinent
Pertinent TRIs are designed to give clients a chance to lead
their therapists to insight that is unique to them and often
quite new (Casement, 1991). In contrast, stereotypic TRIs that are easily
formulated and foremost in thinking, tend to be unhelpful generalizations
(Hedges, 1992).
Because they are personal, pertinent TRIs tend to be
uncomfortable or even painful for clients to hear (Hedges, 1992). Not wanting
to increase their clients’ distress or reveal personal information about
themselves, therapists also find pertinent TRIs difficult to voice. This is especially
true in the area of TL because of its sexual overtones (Danzer,
2018).
One way to increase clients’ comfort is to make pertinent
TRIs inclusive; to link the here-and-now maladaptive habits clients reveal in
therapy with the there-and-then conflicts they have had in life (Safran, et al., 2011). Such TRIs help clients focus less on the embarrassment they are
feeling, and more on a habit they have developed. They also zero in on the
reason for the habit, a reason that makes sense. Such a TRI as “I wonder if you
are being unintentionally seductive with me, just as your brother was with you,”
could help a client move from a subjective feeling state to an objective
cognitive state, while not denying the feeling. It conveys “empathy and
understanding for the position the [client] feels she is in” (Carsky &
Chardavoyne, 2017, p. 403).
Furthermore, this kind of TRI would very likely strike the
client as worth exploring. Problematic interactions in therapy tend to be very
similar to those outside of therapy.
Another way to increase clients’ comfort with pertinent TRIs
is to connect them to the goals they have set. A TRI that reveals how brusque a
client’s remark has come across to the therapist in spite of the client’s goal
to maintain friendships, for example, can move the focus from inappropriate
behavior as such, to why it would be beneficial to replace it with something
that enables goal attainment. It might be worded like “When I try your patience
and you say ‘Whatever’ and change the subject, I feel devalued. Would you like
to find some alternatives?”
A third way to make clients more comfortable is to voice a
TRI that normalizes TL (Danzer, 2018). An example would be
“People tend to be attracted to those they perceive as caring about them. They
even have sexual fantasies about each other. Could that be our case here?”
Inclusive
A simple way to formulate inclusive TRIs is to start with an
observation the client has made about the past and then follow the direction of
the transference to where the past is spilling into the present. For example, “When
you were dependent upon your parents, they went away and left you. When I went
away on vacation, did I remind you of your parents?” This wording offers
clients insight into their past distress while keeping the focus on the
present.
Similarly, inclusive TRIs might link material from a
previous session with what is happening in the present session. For example,
“Last week you spoke of John’s unkindness toward you. I wonder if you are
finding me unkind today.” Or inclusive TRIs might link what clients are saying
about a third party with what they might like to say to their therapist. For
example, “You seem so intent on raking your father over the coals. Would you
also like to do that to me?”
In fact, Gill (1982) recommends routinely including the
words “also” or “in addition” in TRIs. Thus
clients can learn the ancient and deep source of the feelings and impulses they
are re-experiencing. “Remembering and re-experiencing will become organically
blended,” Kahn (1997, p. 59) adds.
At the same time, TRIs do not have to be inclusive to be
pertinent. They need only to refer to core conflicts clients need to resolve in
the here-and-now. They only need to assure clients that the issues they have
come to work on are being dealt with (Gill, 1982). If here-and-now incidents
are actually linked to there-and-then incidents, clients will link them
mentally if not verbally.
A final point is that the criterion of pertinence is
valuable because of our tendency to make what is already known into something
universal and ubiquitous. Instead of being quick to use old insights,
therapists are to tolerate longer exposure to what they do not yet understand.
“And, when they…think [they] recognize something familiar in a [client], [they
are to remain] … receptive to that which is different and new” (Casement, 1991,
p. 29).
Brief and
Simple
As valuable as inclusivity is, however, it must not cancel
out brevity and simplicity. Though complex in that they link key events, TRIs
should focus on one and only one main point. They should not require such
extensive cognitive work that their affective impact is diminished. After all,
the very reason they are mutative is that they are charged with emotion.
To make TRIs simple is to acknowledge the fact that
transference is a relatively simple unconscious phenomenon. The unconscious
mind considers only one characteristic of an object, disregarding all others
and making this feature equal to the whole (Matte Blanco, 1975). Thus Harry
Stack Sullivan is quoted as saying that interpretations should not be longer
than seven words (Swift & Wonderlich, 1990).
For the sake of brevity, therapists might have to divide a
TRI into two successive TRIs. The first would address just the emotional or
cognitive-emotional nature of the client-therapist relationship. The second
would add the extra-therapeutic or pre-therapeutic material. For example, after
processing with the client such a TRI as “I wonder if you are turning me off
because I have hurt you,” the therapist might pause. If the client does not say
anything, the therapist might add, “Could it be that you feel that same hurt
when your wife fails to appreciate your help, as you mentioned last week.”
Similarly, the first TRI might address present or in-session phenomena, and the
second might link the present with the past or with out-of-session phenomena
(Roth, 2001). For example, “Could it be that you are very attracted to me
because I come across as maternal?” would be followed by, “Is it possible that
I remind you of the mother who died when you were a child?”
Respectful
TRIs that are respectful leave clients feeling esteemed even
though they might have developed dysfunctional patterns of relating. They feel
respected for their approach to life and for their struggles to change
(Kiesler, 1982). Furthermore, far from feeling attacked in isolation, they feel
included as collaborators in a process designed to help them change and thereby
gain even more respect.
One of the most common ways to be respectful toward clients
is to ask their permission to consider a certain topic. Thus a TRI
beginning with “Would you be all right with…,” or “Could we look at our
attraction to each other?” conveys a deferential attitude on the part of the
therapist.
For their part, CTRIs should leave therapists feeling
esteemed even though they might have made an error. Thus Hedges (1992) cautions
therapists against being too ready “to assume personal responsibility for the
emerging disruption of untoward feelings” (p. 25). Their doing so could indicate
to clients that they can “[sidestep] completely the more important
interactional component” (p. 25) of the transference phenomenon. Rather, in the
case of TL, they need to explore how both parties might have a
desire for affection, or for an overly supportive relationship, or for total love
(Zilcha-Mano, 2017).
Clients Who Can or Cannot Benefit from TRIs and CTRIs
Distinguishing clients who can benefit from TRIs and CTRIs
from those who cannot is far from easy. However, the following two principles
provide guidance. First, TRIs and CTRIs are appropriate only with clients who
are open to them and ready for them and thus able to benefit from them. Clients
with low self-esteem who are experiencing painful narcissistic injury, for
example, could hardly benefit from having their attention directed to their
contribution to their therapist feeling demeaned.
Second, in general, only clients with at least moderate
ego-strength and generally low-to-medium levels of affective arousal – at
the time – have the capability of benefiting from TRIs and CTRIs.
Though they may be temporarily hurt or angered by what they hear, these clients
can use higher-level defense mechanisms to protect themselves from the worst of
the pain. In particular, they can avoid the use of the splitting defense that
labels them as “all bad” and prevents them from using their cognitive
capacities. They can use their reality-testing function and thus counteract
their tendency to confuse facts with feelings. They can subject perception to
rational scrutiny.
To say this, however, is not to imply that TRIs and CTRIs
are appropriate in any and all sessions with these clients. There will be times
when highly aroused clients simply need to be listened to and allowed to
process their feelings in their own way, even if that takes the entire session.
On the other hand, clients with at least moderate
ego-strength sometimes do not need the entire session to lower affective
arousal. Because they are not in the habit of relying primarily on the
splitting defense, they can return to their more discriminating cognitive
functions. If needed, they can use less primitive defenses such as
intellectualization and rationalization.
At the same time, some clients with moderate ego-strength
and generally low levels of affective arousal, present with embarrassing or
highly sensitive identified problems. If therapists experience these clients as
repeatedly defensive, oppositional, or passive, they should conclude that they
are not ready for TRIs and CTRIs.
Similarly, when clients repeatedly or strongly reject
material, more often than not they are indicating their inability to make
proper use of their cognitive functions. Especially if they are highly
internalizing persons, they could easily experience TRIs as invasive. Instead,
they might benefit from their therapist simply clarifying what they are trying
to say.
It would be the same with highly externalizing clients who are
under great stress. They usually need help with symptom reduction and skill
building rather than insight and relational work. This would be true even if
they had moderate ego-strength. They could benefit from carefully timed and
infrequent TRIs, but only if they are interspersed with plentiful externalizing
interventions, particularly those that are cognitive-behavioral, (Beutler,
2000).
Similarly, clients with a strong need to merge with
idealized others would find it hard to combine their defense mechanism with
CTRIs exposing their therapist’s limitations and flaws, at least until well
into therapy. Simply stated, it is usually necessary for therapists to leave
unchallenged an idealized transference in the beginning phase of therapy
(Kernberg, 1987).
Clients with pronounced limitations justifying dual
diagnoses also find it hard to benefit from TRIs. They lack sufficient
ego-functioning because of such things as significant alcohol and drug
dependence; a well-developed habit of acting out feelings and desires,
especially those that are antisocial or suicidal; and a limited capacity to see
connectedness (Crits-Christoph & Barber, 1991; Pollack & Horner, 1985;
Davanloo, 1990).
Indeed, clients with a borderline personality disorder
deserve careful consideration because of their impulsivity and habit of acting
out their feelings (Denny, et al., 2008). Particularly if they are functioning
at a low level, these clients are likely to perceive TRIs as expected and
deserved counter-assaults. Instead, therapists might simply clarify the way
these clients use splitting and other defenses and are thereby distorting
perceptions.
Occasionally, however, even highly disordered persons can
benefit from interpretations. Franch (1996), for example, writes of a child
with autism and an inability to overcome two-dimensionality and the existence
of a world without meanings. Because the child could experience neither inside
nor outside as such, Franch started to work almost exclusively with his own
countertransference. Fearing that interpreting the child’s transference would
seem invasive to him, he used his own feelings, sensations, fantasies, and
associations to get information about the client’s state of being. He then
assigned meaning to the countertransferential data and communicated it through
CTRIs. Somewhat surprisingly, as Franch communicated the information, the
child’s “frozen” internal world began to “thaw.” His transference had arisen in
response to his therapist’s countertransference interpretations.
Timing of TRIs and CTRIs
Timing depends on clients “inviting” their therapist to
interpret (Joyce, et al., 1995). They generally do so by identifying a
conflict or problem and then elaborating on their distress related to it. They
focus inwardly and stay with their feelings. They attribute personal
significance to the content of a trial-TRI or trial-CTRI and show willingness
to elaborate on it (Sifneos, 1979; Winston, McCullough, & Laikin, 1993).
As with many other principles, however, it may be easier to
identify times when TRIs and CTRIs should not be used.
It would be unwise to use TRIs and CTRIs, for example, if
moderately ego-strong clients were already dealing with a significant past
conflict (Swift & Wonderlich, 1990). Their attention should not be diverted
to a negative therapist-client relationship and its unwholesomeness if they are
already exploring a problematic relationship in the past that is being repeated
in the present. They have identified and owned the destructive pattern they are
using outside the therapeutic setting. They have gotten the point (Pearson,
1995).
Vignette:
She came to therapy sessions very early and stayed
after her therapist ended the sessions. In addition, she focused on the affairs
her husband had had even though he had dealt well with his doing so in the couples’
therapy they had had before she started in her individual work. “Should this be
brought to her attention?” her therapist asked herself. Was there not good
reason to use a very gently worded TRI so that she might consider her own
sexual behavior? She alluded to how she herself had also been unfaithful, but
when her therapist tried to stay with this matter, she brushed it aside more
than once and more than quickly.
At the same time, she gave evidence of significant
emotional instability. She changed topics frequently, hyperventilated
regularly, and spoke of needing to take a break from therapy.
“No,” her therapist decided. “It’s better to stay
close to what she is feeling and doing rather than put TL on the
table. She needs to stabilize and build trust. She is close to revealing
something more fundamentally serious than her adult sexual behavior. Perhaps
it’s her relationship with her son, which she wanted to deal with as her second
goal.”
When her client referred to taking a break a second
time, however, the therapist said, “Yes, we sometimes need to take a break. But
sometimes we need to be brave and look at the possibility of our being
uncomfortable with the person we are with because of our sexual orientation and
theirs. Would you be open to doing that with me? Or at least considering doing
so when you get back?”
Similarly, it would be unwise to use TRIs and CTRIs with
clients experiencing extreme distress related to such things as the death of a
significant other, including a pet; rejection; humiliation; and abuse,
including verbal and/or emotional abuse. A much more effective intervention
would be simple reflective listening.
It would also be unwise to use TRIs and CTRIs when clients
are dealing with material too primitive for language, when they cannot “give
voice” to what they were experiencing. If clients cannot give information, talk
slowly enough to be heard, or speak coherently. TRIs and CTRIs exposing those
phenomena would most likely reinforce their uncomfortable state. More effective
interventions would be attentive silence or short affective responses.
Yet another situation for questioning the wisdom of using
TRIs and CTRIs is when transference is positive. Though positive transference
is a distortion to some extent, it might be necessary for the therapeutic
alliance to develop in clients whose ability to bond is elementary at best. If
their attention is called to their positive transference, it might frighten
them, make them highly self-conscious, or discourage future bonding efforts
(Freud, 1905). As a general rule, positive transference is best left alone if
it does not interfere with therapeutic work or if it is clearly a means of
solidifying and maintaining the therapeutic alliance.
Furthermore, TRIs and CTRIs should not be used too soon,
even under the constraints of brief therapy. They should be used only when
there is evidence of a comfort-level characteristic of a solid therapeutic
alliance (Benner, 1982). In other words, TRIs and CTRIs should ordinarily be
used after more supportive interventions (Gabbard, 1994).
Clients need to feel accepted and valued in their therapy before they can look
at how they have contributed to their failures. This is especially important if
clients are suffering from significant guilt.
In some cases, however, TRIs and CTRIs can be used to establish the therapeutic alliance. They can be used to help clients see that their strongly positive or strongly negative unprocessed attitude toward their therapist is creating an impasse in their therapeutic work (Colli, et al., 2021). TRIs and CTRIs can also be used when the therapeutic alliance or the working alliance has been ruptured (Schaeffer, 2007).
Frequency of TRIs and CTRIs
The answer to the question of frequency of TRIs and CTRIs
begins with a general, research-based rule: since other interventions are often
equally or more appropriate, TRIs and CTRIs should be used infrequently (Piper,
et al., 1991; Hoglend, 1993; Joyce & Piper, 1993). They should be
alternated or interwoven with active listening, explorations, clarifications,
confrontations, and other forms of interpretation (Grunebaum, 1986).
It is especially important to move back and forth between
TRIs or CTRIs and supportive interventions (Bond, et al., 1998) for
personality-disordered individuals. In that way, a solid alliance can be
established and maintained.
How to Decide What to Do with TL and
CTL
How can therapists decide what to do with TL and
CTL that becomes operationalized in their clinical
practice?
How might their practice be affected if they virtually ignored
TL and CTL?
How might clients benefit if therapists made TL and
CTL one focus of their clinical practice?
Do TRIs and CTRIs cause positive therapeutic outcome? Or do they
act as mediators and/or moderators of outcome?
Does research support theories that recommend using TRIs and/or CTRIs to
enable TL and CTL to contribute to positive
outcome?
Does research support theories that recommend not using TRIs
and/or CTRIs in order to avoid a negative outcome?
How scientifically sound is research on what to do with
TL and CTL in actual practice?
Even if that research is less sound than is desirable in general,
are certain findings still worth serious consideration?
Would it be benevolent for therapists to use TRIs and thus invite
clients to collaborate with them to deal with their TL?
Would it be benevolent for therapists to use CTRIs and thus
invite their clients to collaborate with them to deal with their transference
love as it appears in CTL?
The question of what to do with TL and
CTL must be answered, because – like it or not – they act
as powerful, unconscious motivators for both clients and therapists to find
ways to meet their affiliative needs.
We begin with an ethical principle that holds no matter what
therapists decide to do with TL and CTL.
The Principle of Abstinence
To ensure that TL and
CTL do not become a liability, therapists must
refrain from enacting them. “Treatment must be carried out in abstinence,”
(Freud, 1915, p. 163). Both therapists and clients must refrain from any form of
physical expression of their felt need for love and affection. For without
exception, when clients’ “advances [are] returned, it [may be] a great triumph
for [a client or therapist] but a complete defeat for the treatment” (p. 164)
The principle of abstinence is absolute in the case of
erotic, eroticized, and perverse transference (including countertransference
love). But even non-erotic TL that is acted out can cause
confusion and distress in a therapeutic context. Accepting gifts, for example,
on all but a rare occasion can give clients the impression that their therapist
is willing to be in a love-based relationship. Touching clients more often than
absolutely necessary can also “say” to clients that their relationship with
their therapist is virtually the same as with those with whom they and their
clients express their love outside of therapy. As stressed earlier, the four
forms of TL are neither mutually exclusive nor likely to remain
distinct.
Therapists bear primary responsibility for maintaining
abstinence. They must set limits. They must replace their felt
needs and those of their clients with the “counterweight” of a greater love,
either the love of truth and one’s obligations to self and others, or the
passion for healing others (Freud, 1937). Therapists must set firm boundaries.
In some cases, they must go so far as to tell clients that therapy will be
terminated if abstinence cannot be maintained (Kernberg, 1998).
Clinical Choices
Having accepted their responsibility to abstain from
enacting TL and CTL, therapists can choose
to put it aside – virtually ignore it – during sessions with clients.
Therapists most inclined to choose this option are those whose needs to be
admired and respected trump their willingness to be vulnerable with their
clients (Charles, 1999).
Of course, this first choice can also be based on the
theoretical position that non-analytic therapists are insufficiently prepared
to deal directly with TL. “A [client] sharing sexual feeling for
a therapist can be one of the most difficult experiences for both parties. Such
experiences combine the anxiety of intense emotional expression and negotiation
of a relationship while affirming professional and personal boundaries,”
(Malark, 2017, p. 418; McWilliams, 2004). Furthermore, there are other ways to
help clients deal with unconscious desires and motives related to their
affiliative issues. Similarly, there are other, purely personal and/or
collegial ways to process CTL.
In any case, therapists choosing to ignore TL that arises in their clinical work should seriously consider engaging in one or more of the following: evaluating between sessions the impact of transference love during sessions; using interventions other than interpretations, especially standardized assessments (Churchill & Ridenour, 2019) to discover and address TL that becomes problematic; dealing with countertransferential issues in their own personal therapy; and/or consulting with supervisors or experienced colleagues. The appropriateness of the latter might even head the list in light of how difficult it is to assess the impact of TL in the actual setting. In fact, valid and reliable assessment by an involved
clinician himself might even be “impossible” (Churchill & Ridenour, 2019).
The value of dealing with transference and countertransference love in one’s own personal therapy and with one’s supervisor cannot be overestimated. Research reveals that therapists, especially those still in training, feel most comfortable talking about sexual attraction with their therapist, followed by their supervisor (Williams, et al., 2016). Research also reveals how difficult it is to assess the impact of TL and CTL in the actual therapy setting. In fact, valid and reliable assessment by an involved clinician himself might even be impossible (Churchill & Ridenour, 2019).
Therapists’ second choice is to draw clients’ attention to
TL and invite them to co-process it during sessions by using
TRIs but not CTRIs. Doing so is based on the theoretical position that
abstinence from enactment should not mean “deprivation of
everything that the [client] desires” (Freud, 1915, p. 163). It should not result
in therapists’ becoming cold, aloof, or distant, for these reactions can imply
that TL is unacceptable, even disgusting. It may even reinforce
the belief of many clients that they are truly unlovable
(Gerrard, 1999).
Therapists who choose to use TRIs but not CTRIs base their
decision on theory that holds that therapists’ intrapsychic processing of their
countertransference is usually sufficient to counteract enactment of it unless
it is extremely subtle or unusually potent. Furthermore, using CTRIs can give
clients the impression that their therapist is more interested in himself or
herself than in them (Schaeffer, 1998).
In addition, pinning down the exact nature of
CTL is generally more difficult for therapists than doing
so with TL. It is hard to meet the criterion of emotional
immediacy with CTRIs. Even if it is met, CTRIs can be meaningless to clients in
that they may be inaccurate or incomplete. If countertransference is especially
negative, it is also hard to meet criteria of calmness, neutrality, and
tentativeness. Thus CTRIs can damage clients because of prosody: tone, volume,
inflection, and accompanying body language (Schaeffer, 1998).
Therapists who choose to use just TRIs also base their
decision on theory supportive of their relationship to positive outcome. TRIs foster
that outcome because they build rapport as well as strengthen and repair the
therapeutic alliance. Furthermore, TRIs that clearly refer to clients’
here-and-now core conflicts, and/or connect therapists to parents and siblings,
contribute to treatment efficacy. Clients also benefit from TRIs that link
their affiliative needs and desires with the responses of others, beginning
with those of their therapist. Furthermore, TRIs are easily combined with
non-transferential interventions, such as reflective listening, explorations,
clarifications, questions, and even gentle confrontations. These interventions,
in turn, have been found to be very efficacious (Schaeffer, 1998).
Finally, therapists who are adequately prepared to perform
the subtasks related to formulating and verifying TL are in a
position to use TRIs to help clients with a variety of mental health diagnoses.
Unless clients’ goals are purely personal, therapists can use the therapeutic
setting to help clients attain those goals of relating to others in truly
loving ways. They can make the therapeutic setting a safe place to do that
difficult work by putting clients’ TL into words and inviting
their clients to collaborate with them so that they understand what they are
bringing to their sessions. Therapists can become safe persons with whom
clients can learn how to meet their affiliative needs in mature and wholesome
ways – loving themselves along with nourishing adult-adult affiliative relationships
– perhaps for the first time in their lives (Schaeffer, 2007).
Therapists’ third choice is to use both TRIs
and CTRIs. It is based on the theoretical position that both
TL and CTL deserve to reveal their
potential for helping clients resolve their past-based psychological conflicts
and meet their present affiliative needs. Therapists who adhere to this
position consciously choose to “sink into” their own and their clients’
affiliative phenomena without “drowning” in them (Gabbard, 1994). They work to
increase their own and their clients’ comfort level with viewing themselves as
human beings complete with erotic – no less than non-erotic – desires. They
have by nature both pathological and non-pathological propensities to meet
their affiliative needs. Therefore, they are willing to incorporate TRIs and
CTRIs related to affiliation into their work. They are willing to risk making
therapy overly relational as well as intrapsychic.
Indeed, using TRIs and CTRIs makes explicit the potential both
TL and CTL have toward meeting affiliative
needs in truly wholesome ways. Doing so means directly helping clients replace
mindless and unproductive action, namely simple reenactment (Freud, 1915), with
conscious and productive processing of affiliative needs. They can thereby
experience a generative shift leading to a deeper level of self-experience
(Slochower, 1999). They can experience themselves and others as profoundly
good, genuinely desirable, and actually loved (Schaeffer, 2007). They can move
from “I love you mainly because you love me,” and “I love you because I need
you,” to “I am loved because I love myself,” and “I need you because I love you”
(Fromm, 1976).
In addition, using TRIs and CTRIs enables therapists to help
clients realize that with TL and CTL comes
the opportunity to mourn, perhaps for the first time, the loss of early
parental love. Their grief is appropriate because what they always wanted from
parental figures was and still is unattainable (Maroda, 2000).
They must mourn not being able to go back in time to become infants. They must
replace that desire, first and foremost, with providing that love for
themselves. By truly loving themselves, they will then be able to enter into
unselfish, loving, and mutually satisfying relationships with others.
The decision to make the second and third choices, of
course, also calls for a nuanced approach made possible only by weighing the
following pros and cons based on extant research findings.
Research Findings
While quantitative, qualitative, and quantitative-qualitative research regarding the use of TRIs and CTRIs is impressive, it is important to keep in mind that it is limited in both quality and quantity. There have been relatively few scientifically sound studies of TRIs and even fewer of CTRIs according to current standards. Some of these studies were neither adequately designed nor methodologically sound. Some did not use control groups or sufficiently large populations. Most were not replicated or longitudinal. Thus it is not possible to draw firm conclusions from most studies conducted thus far. At the same time, it is possible to use research data to inform treatment decisions.
TRIs and CTRIs do not cause positive therapeutic
outcome. Rather, they act as mediators and moderators of outcome (Schaeffer,
1998).
Acting as mediators, TRIs can enable clients to address the issue
of their present affiliative needs by identifying past conflicts related to
them (Malan, 1976; Marziali, 1984; Luborsky, et al., 1988). TRIs can help
clients disconfirm pathological beliefs resultant from childhood trauma
(Fretter, et al., 1994).
Indiscriminate use of TRIs, however, can distract clients
from focusing on the issues they explicitly brought to therapy (Grunebaum, 1986).
Acting as moderators, too many TRIs – or TRIs used inappropriately – decrease
the benefit of focusing on the non-transferential issues clients identify as
important to them when they seek therapy.
TRIs can contribute indirectly to negative outcome if they are
used with inappropriate clients or used too frequently (Piper, et al., 1993;
Grunebaum, 1986). At the same time, accurate, sensitively timed, and
occasionally used TRIs can make an indirect contribution to successful outcome
by positively affecting correlates of that outcome: rapport building; the
therapeutic alliance; continuance in therapy; and the working alliance
(Fretter, et al., 1994; Luborsky, et al., 1988; Foreman & Marmar, 1985;
Piper, et al., 1993; Joyce & Piper, 1993).
Careful use of TRIs can contribute to successful outcome with a
variety of diagnostic categories and non-diagnostic populations (McCullough
& Winston, 1991).
Though little research has been conducted on the use of CTRIs as
such, therapeutic success for clients correlates with early-session
interpretations that accurately link participants’ needs and wishes with how
others respond. CTRIs can lead to successful outcome because of clients’
increased awareness of the contribution their behavior makes to their
therapist’s well-being or lack thereof (Crits-Cristoph, et al., 1998). Thus,
CTRIs are mediators of successful outcome and moderators of the level of that
outcome.
CTRIs have also been found to be mediators of positive outcome in
that they draw clients’ attention to universal human vulnerability as well as
to the capacity for self-regulation (Beard, 1992) and for reflective thought
rather than mindless action (Feldman, 1997).
CTRIs have also been found to perform a useful modeling function.
“The willingness to self-disclose on the [therapist’s] part facilitates
self-disclosure by the [client], and therefore productive dialectical
interchange between [therapy participants] is maximized” (Renik, 1993, p. 529).
Thus, CTRIs are mediators and moderators of successful outcome.
Clients are usually aware of their therapist’s feelings, whether
communicated or not (Racker, 1968; Crowley, 1988). Using CTRIs is one way of
processing what clients are already aware of.
If therapists do not process their countertransferential feelings
during sessions; that is, do not name them, validate them, or give them minimal
expression; it is highly probable that they will act them out in silence,
withdrawal, coldness, distancing (McDougall, 1978; Danzer, 2018), fatigue, or
inappropriate timing, tact, or tone (Jacobs, 1986; Myerson, 1993).
Unaddressed countertransference conflicts are also likely to
result in acting-in, taking such forms as depression and somatization. In fact,
Boyer (1961) found that unaddressed countertransference conflicts are the major
reason for therapeutic failure.
By sharing countertransference, therapists increase the
probability that they will become enlightened about themselves, their clients,
and the work their clients need to do in therapy. Therapists’ thoughts,
sensations, and feelings act as mirrors reflecting what clients perceive that their
therapists are experiencing (Little, 1957), even as therapists are acting as
mirrors for their clients (Casement, 1991). Thus, through countertransference
that is shared, clients are in a position to enlighten
therapists as to what they as clients want to accomplish in therapy (Ehrenberg,
1996).
Sharing countertransference has a powerful modeling effect
(Little, 1957; Bollas, 1983; DeLaCour, 1985; Bandura, 1971). It demonstrates
for clients appropriate ways of dealing with problematic feelings in close,
interpersonal settings (Bollas, 1983). When countertransference is shared,
clients learn how to acknowledge and care for the archaic or unconscious
(Loewald, 1986); how to be honest (Searles, 1979); and how to struggle with
feelings, frustrate them, manage them, contain them, explore them, and
eventually integrate them (McDougall, 1978). CTRIs teach clients how to be
emotionally available (Viederman, 1991).
CTRIs can contribute to the formation and strengthening of the
therapeutic alliance (Kiesler, 1982; Alpert, 1992). They offer concrete and
convincing evidence of therapists’ attunement to their clients (Stolorow,
1993).
TRIs and CTRIs can be cost-effective, even though therapeutic
outcome does not depend on their use (Gassner, et
al., 1982; Fretter, et al., 1994; Weiss & Sampson, 1986; Silberschatz, et
al., 1986; Schaeffer, 2007).
A given intervention such as using TRIs and/or CTRIs can affect
outcome, but not determine it, because all therapeutic interventions combined
account for only 40% of successful outcomes (Lambert, 2001).
Conclusion
TL and CTL arising in
therapy are ubiquitous double-edged swords. They can be harmful if not
recognized and regarded as phenomena that reveal our innate, life-long needs to
love and be loved.
At the same time, they can be beneficial if carefully worked
with in the light of their being potential mediators and moderators of healing
long-held psychological pain. They can facilitate a generative shift in the
course of which clients and therapists experience themselves as innately good,
genuinely desirable, actually loved, and able to love others in developmentally
appropriate ways.
Thus we are wise to weigh the forewarning of Gerrard (1999):
“Until and unless there can be felt moments of love for the [client] by the
therapist, the [client] is not able to develop fully. It is only when [he or
she] can arouse [the therapist’s] deepest loving feelings (not empathy) that
[therapists] can hope for a truly positive outcome from [their] work” (p. 30).
We are also wise to reflect on the attestation of Rabin
(2003): TL and CTL that are processed well
can make therapy a truly benevolent experience. It can enable clients to deal
with difficult situations outside of therapy.
And we are wise to ponder the findings of Bachant &
Adler (1997): if clients are able to tolerate passionate love, they will
undergo a maturation that would not have occurred otherwise. They will learn
the deepest lessons of the heart.
And their therapists will also.
References
Alpert, M. C. (1992). Accelerated empathic therapy: A new short-term dynamic psychotherapy. International Journal of Short-Term Psychotherapy, 7, 133-156.
Arlow, J. (1985). Some technical problems of countertransference. Psychoanalytic Quarterly, 54, 164-174.
Audet, C. (2011). Client perspectives of therapist self-disclosure: Violating boundaries or removing barriers? Counseling Psychology Quarterly, 24, 85-100.
Bacal, H. A. (1990). Optimal responsiveness and the specificity of self-object experience. In H. A. Bacal (Ed.), Optimal responsiveness: How therapists heal their patients (pp. 141-170). Jason Aronson.
Bachant, J., & Adler, D. (1997). Transference: Co-constructed or brought to the interaction? Journal of the American Psychoanalytic Association, 45, 1097-1120.
Bandura, A. (1971). Psychological modeling. Aldine-Atherton.
Beard, D. K. (1992). Somatic knowing with the psychosomatic patient: An answer in kind. [Unpublished doctoral dissertation]. California School of Professional Psychology.
Bennett, K., & Clark, E. (2021). Crossing guardians: signaling and safety in queer and trans therapist/patient dyads. Psychoanalytic Psychology, 38, 216-222.
Beutler, L. E. (2001). David and Goliath: When empircal and clinical standards of practice meet. American Psychologist, 55(9), 997-1007.
Bird, B. (1922). Notes on transference: Universal phenomenon and the hardest part of analysis. Journal of the American Psychoanalytic Association, 20, 267-301.
Blum, H. P. (1997). Clinical and developmental dimensions of hate. Journal of the American Psychoanalytic Association, 45(2), 359-375.
Bollas, C. (1983). Expressive use of the countertransference. Contemporary Psychoanalysis, 19, 1-34.
Bollas, C. (1987). The shadow of the object: Psychoanalysis of the unthought known. Free Association Books.
Bond, M., Banon, E., & Greneier, M. (1998). Differential effect of interventions on the therapeutic alliance with patients with personality disorders. Journal of Psychotherapy Practice and Research, 7, 301-318.
Boyer, L. B. (1997). The verbal squiggle game in treating the seriously disturbed patient. In V.D. Volken and S. Akhtar (Eds.), The seed of madness (pp. 155-176). International Universities Press.
Brenner, C. (1982). The mind in conflict. International University Press.
Brodbeck, H. (1995). The psychoanalyst as participant and observer in the psychoanalytic process: Some thoughts on countertransference from a constructionist perspective. Psychoanalysis and Contemporary Thought,18, 531-558.
Carsky, M., & Chardavoyne, J. (2017). Transference focused psychotherapy and the language of action. Psychoanalytic Psychology, 34, 397-403.
Casement, P. (1991). Learning from the patient. The Guilford Press.
Celenza, A. (2017). Lessons on or about the couch: What sexual boundary transgressions can teach us about everyday practice. Psychoanalytic Psychology, 34, 157-162.
Celenza, A. (2021). Erotic transferences and countertransferences in sexual boundary violations: An Interview with Andrea Celenza. In A. Steinberg, J. Alpert, & C. Courtois, (Eds.). Sexual boundary violations in psychotherapy: Facing therapist indiscretions, transgressions, and misconduct, (pp. 69-89). American Psychological Association.
Charles, M. (1999). The promise of love: A view among women. Psychoanalytic Psychology, 16, 254-273.
Chasseguet-Smirgel, J. (1984). Creativity and perversion. Free Association Books.
Chodorow, N. (1978). The reproduction of mothering: Psychoanalysis and the sociology of gender. University of California Press.
Churchill, H., & Ridenour, J. (2019). Coming together through falling apart. Rorschachiana, 40(2), 151-168.
Colli, A., Gagliardini, G., & Guillo, S. (2022). Countertransference responses mediate the relationship between patients; overall defense functioning and therapists’ interventions. Psychotherapy Research, 32(1):45-58. doi: 10.1080/10503307.2021.1884768
Cooper, A. M. (1987). Changes in psychoanalytical ideas: Transference interpretation. Journal of the American Psychoanalytical Association, 35, 77-98.
Cooper, S. (1993). Interpretive fallibility and the psychoanalytic dialogue. Journal of the American Psychoanalytic Association, 41(1), 95-123.
Covington, C. (1996). Purposive aspects of the erotic transference. Journal of Analytical Psychology, 41, 339-352.
Crits-Christoph, P., & Barber, J. P. (Eds.). (1991). Handbook of short-term dynamic psychotherapy. Basic Books.
Crowley, R. M. (1988). Human reactions of analysts to patients. In B. Wolstein (Ed.), Essential papers on countertransference (pp.84-90). New York University Press.
Dalenberg, C. (2000). Countertransference and the treatment of trauma. American Psychological Association.
Danzer, G. (2018). Therapeutic self-disclosure of religious affiliation: A critical analysis of theory, research, reality, and practice. Psychology of Religions and Spirituality, 1-6.
Davanloo, H. (1990). Unlocking the unconscious. Wiley.
Davies, J. M. (1994). Love in the afternoon: A relational reconsideration of desire and dread in the countertransference. Psychoanalytic Dialogues, 4(2), 153-170.
DeLaCour, E. P. (1985). Aspects of transference interpretation. Smith College Studies in Social Work, 56, 1-14.
Denney, R., Aten, J., & Gingrich, F. (2008). Using spiritual self-disclosure in psychotherapy. Journal of Psychology and Theology, 36, 294-302.
Deutsch, H. (1926). Occult processes during psychoanalysis. In G. Devereux (Ed.), Psychoanalysis and the occult (pp.133-146). International Universities Press.
Diamond, D. (2018). Changes in Object Relations in Psychotherapy with Schizophrenic Patients: Commentary on Carsky and Rand (2018). Psychoanalytic Psychology, 35, 410-414.
Dosamantes, I. (1992). The intersubjective relationship between therapist and patient: A key to understanding denied and denigrated aspects of the patient's self. The Arts & Psychotherapy, 19, 359-365.
Dreher, M., Mengele, U., Rainer, K., & Kammerer, A. (2001). Affective indicators of the psychotherapeutic process: An empirical case study. Psychotherapy Research 11(1), 99-117.
Ecker, B., Hulley, L., & Ticic, R. (1996). Depth-oriented brief therapy. Jossey-Bass.
Ecker, B., Ticic, R., & Hulley. L. (2012). Unlocking the emotional brain. Routledge.
Ehrenberg, M. F., Hunter, M. A., & Elterman, M. F. (1996). Shared parenting agreements after marital separation: The roles of empathy and narcissism. Journal of Consulting and Clinical Psychology, 64(4), 808–818.
Eickhoff, F. W. (1979). Panel reports: Technical management of highly erotic transference. International Journal of Psycho-Analysis, 78, 587-591.
Elise, D. (2019). Creativity and the erotic dimensions of the analytic field. Routledge.
Epstein, L. (1977). The therapeutic function of hate in the countertransference. Contemporary Psychoanalysis, 13, 442-461.
Etchegoyen, R. H. (1978). Some thoughts on transference perversion. International Journal of Psycho-Analysis, 59, 45-53.
Fast, I. (1992). Developments in gender identity: Gender differentiation in girls. International Journal of Psycho-Analysis, 60, 443-453.
Faulkner, W. (1929). The Sound and the Fury: and As I Lay Dying. Modern Library.
Federmeier, K. D., & Kutas, M. (2002). Picture the difference: Electrophysiological investigations of picture processing in the two cerebral hemispheres. Neuropsychological, 40, 730-747.
Feldman, M. (1997). Projective identification: The analyst's involvement. International Journal of Psycho-Analysis, 78, 227-241.
Ferenczi, S. (1909). Sex in psychoanalysis. Basic Books.
Field, N. (1989). Listening with the body: An exploration in the countertransference. British Journal of Psychotherapy, 5(4), 512-522.
Foreman, S. A., & Marmar, C. R. (1985). Therapist actions that address initially poor therapeutic alliances in psychotherapy. American Journal of Psychiatry, 142, 922-926.
Franch, N. (1996). Transference and countertransference in the analysis of a child with autistic nuclei. International Journal of Psycho-Analysis, 77, 773-786.
Fretter, P. B., Bucci, W., Broitman, J., Silberschatz, G., & Curtin, J. T. (1994). How the patients' plan relates to the concept of transference. Psychotherapy Research, 4(1), 58-72.
Freud, S. (1905). Fragment of an analysis of a case of hysteria. (Std. Ed., 7). 1-122. Hogarth Press.
Freud, S. (1912). The dynamics of transference. (Std. Ed., 12) 99-108. Hogarth Press.
Freud, S. (1915). Observations on transference-love. (Std Ed., 12) 157-171. Hogarth Press.
Freud, S. (1937). Analysis terminable and interminable. (Std Ed., 23) 209-253. Hogarth Press.
Freud, S. (1940). An outline of psychoanalysis. (Std Ed., 23) 139-207. Hogarth Press.
Freud, S., & Jung, C. G. (1974). The Freud/Jung letters. W. McGuire (Ed.) and R. Manheim & R. Hull (Trans.). Princeton University Press.
Fromm, E. (1976). The art of loving. Unwin.
Gabbard, G. O. (Ed.). (1989). Sexual exploitation in professional relationship. American Psychiatric Press.
Gabbard, G. O. (1994). Sexual excitement and CTL in the analyst. Journal of the American Psychoanalytic Association, 42, 1083-1106.
Gabbard, G. O. (1996). Therapeutic approaches to erotic transference. In F. Flack (Ed.), The Hatherleigh guide to psychotherapy (pp. 231-247). Hatherleigh Press.
Gabbard, G. O. (2001). What can neuroscience teach us about transference? Canadian Journal of Psychoanalysis, 9(1), 1-18.
Gassner, S., Sampson, H., Weiss, J., & Brumer, S. (1982). The emergence of warded-off contents. Psychoanalysis and Contemporary Thought, 5(1), 55-75.
Gazzaniga, M. (Ed.) (1995). The cognitive neurosciences. The MIT Press.
Gelso, C. J., & Hayes, J. A. (1998). The psychotherapy relationship. John Wiley & Sons, Inc.
Gerrard, J. (1999). Love in the time of psychotherapy. In D. Mann (Ed.), Erotic transference and countertransference: Clinical practice in psychotherapy (pp. 29-41). Routledge.
Gill, M. M. (1982). Analysis of transference (Vol.1). International Universities Press.
Gorkin, M. (1997). Countertransference in cross-cultural psychotherapy. In R. Perez-Foster, M. Moskowitz, & R. A. Javier (Eds.), Reaching across boundaries of culture and class: Widening the scope of psychotherapy (pp. 159-176). Jason Aronson.
Gorney, J. W. (1979). The negative therapeutic reaction. Contemporary Psychoanalysis, 15, 288-337.
Greenacre, P. (1954). The role of transference: Practical considerations in relation to psychoanalytic therapy. Journal of the American Psychoanalytic Association, 2, 671-684.
Grigsby, J., & Stevens, D. (2000). Neurodynamics of personality. Guilford.
Grinberg, L. (1997). Is the transference fear by the psychoanalyst? International Journal Psycho-Analysis, 78, 1-14.
Grunebaum, H. (1986). Harmful psychotherapy experience. American Journal of Psychotherapy, 40, 165-176.
Heath, S. (1991). Dealing with the therapist's vulnerability to depression. Jason Aronson.
Hedges, L. E. (1992). Interpreting the countertransference. Jason Aronson.
Herron, W. G., & Rouslin, S. (1982). Issues in psychotherapy. Orgin.
Hinshelwood, R. (1999). Countertransference. International Journal of Psycho-Analysis, 80, 797-818.
Hoglend, P. (1993). Transference interpretations and long-term change after dynamic psychotherapy of brief to moderate length. American Journal of Psychotherapy, 47, 494-507.
Holmes, D. E. (1992). Race and transference in psychoanalysis and psychotherapy. International Journal of Psycho-Analysis, 73(1), 1-11.
Hubble, J. P. (1999). Novel drugs for Parkinson's disease. The Medical Clinics of North America, 83, 525-536.
Isakower, O. (1963). Minutes of the New York psychoanalytic institute faculty meeting, October 14. [Unpublished].
Jacobs, T. J. (1986). On countertransference enactments. Journal of the American Psychoanalytical Association, 34, 289-307.
Joseph, B. (1987). Projective identification: Clinical aspects. In J. Sandler (Ed.), Projection, identification, and projective identification (pp. 65-76). International Universities Press.
Joyce, A. S., & Piper, W. E. (1993). The immediate impact of transference interpretation in short-term individual psychotherapy. American Journal of Psychotherapy, 47, 508-526.
Joyce, A. S., Duncan, S. C., & Piper, W. E. (1995). Task analysis of “working” responses to dynamic interpretation in short-term individual psychotherapy. Psychotherapy Research, 5(1), 49-62.
Jung, C. G. (1946). The psychology of the transference. Collected works, Vol. 16. Bollingen.
Kahn, M. (1997). Between therapist and client: The new relationship (Rev. ed.). W. H. Freeman & Co.
Kaplan, L. (1991). Female perversions: The temptations of Madame Bovary. Doubleday.
Kernberg, O. F. (1987). An ego psychology-object relations theory approach to the transference. Psychoanalytic Quarterly, 56, 97-221.
Kernberg, O. F. (1994). Love in the analytic setting. Journal of the American Analytic Association, 42, 1137-57.
Kernberg, O. W. (1975). Borderline conditions and pathological narcissism. Jason Aronson.
Kernberg, P. (1998). Sexuality in the analysis of adolescents: Its impact on the transference-countertransference. International Journal of Psycho-Analysis, 79(2) 366-7.
Kiesler, D. J. (1982). Confronting the client-therapist relationship in psychotherapy. In J. C. Anchin & D. J. Kiesler (Eds.), Handbook of interpersonal psychotherapy (pp. 280-295). Pergamon Press.
Lambert, M. J. (2001). The effectiveness of psychotherapy. Colorado Psychological Association Bulletin, 34, 9, 11, 15.
Langs, R. (1979). The interactional dimension of countertransference. In L. Epstein & A. J. Feiner (Eds.), Countertransference (pp. 71-103). Jason Aronson.
Laplanche, J. (1997). The theory of seduction and the problem of the other. The International Journal of Psychoanalysis, 78, 653-666.
Lear, J. (1993). An interpretation of transference. International Journal of Psycho-Analysis, 74, 739-755.
Levin, F. (1997). Integrating some mind and brain views of transference: The phenomena. Journal of the American Psychoanalytic Association, 45, 1121-1151.
Lewis, O. (2024). Countertransference teaching: The challenge of going beyond literature, a novel approach. Medical Research Archives, 12(1), 1-7. doi: https://doi.org/10.18103/mra.v12i1.4926
Little, M. (1957). 'R' – The analyst's total response to his patient's needs. International Journal of Psycho-Analysis, 38, 240-254.
Loewald. H. W. (1986). Transference-countertransference. Journal of the American Psycho-analytic Association, 34, 275-289.
Luborsky, L., Crits-Christoph, P., Mintz, J., & Auerbach, A. (1988). Who will benefit from psychotherapy? Basic Books.
Lyons-Ruth, K. (2000). I sense that you sense that I sense…: Sander's recognition process and the specificity of relational moves in the psychotherapeutic setting. Infant Mental Health Journal, 21, 85-98.
Malan, D.H. (1976). Toward the validation of dynamic psychodynamic psychotherapy. Plenum Press.
Malark, A. (2017). Sexuality, religion, and atheism in psychodynamic treatment. Psychology of Sexual Orientation and Gender Diversity, 4, 412-421.
Mandal, M. K., & Ambady, N. (2004). Laterality and universality of facial expressions of emotions: The interface. Behavioural Neurology, 15, 23-34.
Mann, D. (1997). Psychotherapy: An erotic relationship. Routledge.
Mann, D. (1999). Clinical practice in psychotherapy. In D. Mann (Ed.), Erotic transference and countertransference (pp. 1-25). Routledge.
Maroda, K. (1995). Projective identification and countertransference interventions: Since feeling is first. Psychoanalytic Review, 82(2), 229-247.
Marziali, E. A. (1984). Prediction of outcome of brief psychotherapy from therapist interpretive interventions. Archives of General Psychiatry, 41, 301-304.
Marziali, E. A., & Sullivan, J. M. (1980). Methodological issue in the content analysis of brief psychotherapy. British Journal of Medical Psychology, 53, 19-27.
Mathew, R. J., Wilson, W. H., Turkington, T. G., & Coleman, R. E. (1998). Cerebellar activity and disturbed time sense after THC. Brain Research, 792(2), 183-189.
Matte Blanco, I. 1975). The unconscious as infinite sets: An essay in bi-logic. Duckworth.
McCullough, L., & Winston, A. (1991). The Beth Israel psychotherapy research program. In L. Beutler & M. Crago (Eds.). Psychotherapy research: An international review of programmatic studies (pp. 525-533). American Psychological Association Press.
McDougall, J. (1978). Primitive communication and the use of countertransference. Contemporary Psychoanalysis, 14, 173-209.
McWilliams, N. (2004). Psychoanalytic Psychotherapy: A practitioner’s guide. Guilford Press.
Meares, R., Stevenson, J., & Comerford, A. (2005). Distinct pattern of P3a event and related in borderline personality disorders. NeuroReport, 16, 289-293.
Meissner, W. (1996). The therapeutic alliance. Yale University Press.
Menninger, K. (1942). Love against hate. Harcourt, Brace.
Morris, H. (2012). Constituting the ethics of psychoanalysis: Observations on “Observations on transference love,” the story. [Paper presented on Panel on Ethics], Boston Psychoanalytic Society and Institute.
Myerson, P. (1993). Listening for the effects of psychoanalytic interventions. Contemporary Psychoanalysis, 29, 397-417.
Nissen, H., Dahl, H., & Hoglend, P. (2020). Patient factors predict therapist’s emotional countertransference differently depending on whether therapists use transference work in psychodynamic therapy. Psychotherapy Research, 3, 3-14.
Ogden, T. H. (1982). Projective identification and psychotherapeutic technique. Jason Aronson.
Ogden, T. H. (1994). The concept of interpretive action. Psychoanalytic Quarterly, 63(2), 219-245.
Pally, R. (1997). Developments in neuroscience: II How the brain actively constructs perceptions. International Journal of Psycho-Analysis, 78, 1021-1030.
Pearson, M. (1995). Problems with transference interpretations in short-term dynamic therapy. British Journal of Psychotherapy, 12, 37-48.
Person, E. S. (1995). The erotic transference in women and in men: Differences and consequences. Journal of the American Psychoanalytic Association, 43, 159-180.
Pick, I. B. (1997). Working through in the countertransference. In R. Schafer (Ed.), The contemporary Kleinians of London (pp. 348-367). International University Press.
Piper, W. E., Azim, H. F. A., Anthony, J., & McCallum, M. (1991). Transference interpretations, therapeutic alliance, and outcome in short-term individual psychotherapy. Archives of General Psychiatry, 48, 946-957.
Piper, W. E., McCallum, M., Azim, H. F. A., & Joyce, A. S. (1993). Understanding the relationship between transference interpretation and outcome in the context of other variables. American Journal of Psychotherapy, 47, 479-493.
Pollack, J., & Horner, A. (1985). Brief adaptation-oriented psychotherapy. In A. Winston (Ed.).Clinical and research issues in short-term dynamic psychotherapy (pp. 58-79). American Psychiatric Press.
Pope, K. S., Sonne, J. L., & Holroyd, J. (1994). Sexual feelings in psychotherapy: Explorations for therapists and therapists in training. Washington, DC. American Psychological Association.
Rabin, H. (2003). Love in the countertransference: Controversies and questions. Psychoanalytic Psychology, 20(4), 677-307.
Racker, H. (1953). A contribution to the problem of countertransference. International Journal of Psycho-Analysis, 34, 313-324.
Racker, H. (1968). Transference and countertransference. International Universities Press.
Renik, O. 1993. Analytic interaction: conceptualizing technique in the light of the analyst's irreducible subjectivity. Psychoanalytic Quarterly, 62, 518-532.
Roth, P. (2001). Mapping the landscape: Levels of transference interpretation. The International Journal of Psychoanalysis, 82, 533-543.
Russ, H. (1999). Leaving chastity behind. Psychoanalytic Psychology, 16(4), 605-616.
Safran, J. D., Muran, J. C., & Eubanks-Carter, C. (2011). Repairing alliance ruptures. Psychotherapy, 48(1), 80-87.
Sandler, J. (1976). Countertransference and role responsiveness. International Review of Psychoanalysis, 3, 43-47.
Scaer, R. C. (2005). The trauma spectrum: Hidden wounds and human resiliency. W. W. Norton.
Schaeffer, J. A. (1998). Transference and countertransference interpretations: Harmful or helpful in short-term dynamic therapy? American Journal of Psychotherapy, 52(1), 1-17.
Schaeffer, J. A. (2007). Transference and countertransference in non-analytic therapy: Double-edged swords. University Press of America, Inc.
Schafer, R. (1977). The interpretation of transference and the conditions for loving. Journal of the American Psychoanalytic Association, 25, 335-362.
Schafer, R. (1983). The analytic attitude. Basic Books.
Schafer, R. (1997). Vicissitudes of remembering in the countertransference: Fervent failure, colonization and remembering otherwise. International Journal of Psycho-Analysis, 78, 1151-1163.
Schaverien, J. (1997). Men who leave too soon: Reflections on the erotic transference and countertransference. British Journal of Psychotherapy 14, 3-16.
Schoenewolf, G. (2004). 111 common therapeutic blunders. Jason Aronson, Inc.
Schore, A. N. (1994c). Affect regulation and the origin of the self. Lawrence Erlbaum.
Schore, A. N. (2003a). Affect dysregulation and disorders of the self. W. W. Norton.
Schore, A. N. (2003b). Affect regulation and the repair of the self. W. W. Norton.
Schwaber, E. (1990). Interpretation and the therapeutic action of psychoanalysis. Journal of Psycho-Analysis, 71, 229-240.
Searles, H. (1975). The patient as therapist to his analyst: Nontransference. In P. Giovacchini (Ed.), Tactics and techniques in psychoanalytic therapy: Countertransference (Vol. II) (pp. 95-151). Jason Aronson.
Searles, H. (1979). Countertransference and related subjects in selected papers. International Universities Press.
Shedler, J. (2021). The personality syndromes. In R. Feinstein (Ed.), A primer on personality Disorders: Multi-theoretical Viewpoints. Oxford University Press.
Sifneos, P. E. (1979). Short term dynamic psychotherapy: Evaluation and technique (2nd ed.). Plenum Press.
Silberschatz, G., Fretter, P. B., & Curtin, T. (1986). How do interpretations influence the process of psychotherapy? Journal of Consulting and Clinical Psychology, 54, 646-652.
Silverman, D. (2019). Book review. Psychoanalytic Psychology, 37, 1-4.
Slavin, J., Rahmani, M., & Pollock, L. (1998). Reality and danger in psychoanalytic treatment. Psychoanalytic Quarterly, 67, 191-217.
Slochower, J. (1999). Erotic complications. International Journal of Psycho-Analysis, 80, 1119-1130.
Smith, H. (1990). Cues: The perceptual edge of the transference. International Journal of Psycho-Analysis, 71, 219-228.
Smith, H. (2000). Countertransference, conflictual listening, and the analytic object relationship. Journal of the American Psychoanalytic Association, 48, 95-128.
Spence, D., Shapiro, D., & Zaidel, E. (1996). The role of the right hemisphere in the physiological and cognitive components of emotional processing. Psychophysiology, 33, 112-122,
Springer, A. (1996). Female perversion: Scenes and strategies in analysis and culture. Journal of Analytical Psychology, 41, 325-338.
Stacy, S. C. (1998). Exploring the role of psychic conflict and development deficit in erotically charged transferences. Dissertation Abstracts International: Section B: The Sciences & Engineering, 58(12; B), 6828.
Stamm, B. H. (1995). Secondary traumatic stress: Self-care issues for clinicians, Researchers, and Educators. The Sidran Press.
Stark, M. (1994). Primer on working with resistance. Jason Aronson.
Stoller, R. (1975). Perversion: The erotic form of hatred. Pantheon.
Stolorow, R. D. (1993). An intersubjective view of the therapeutic process. Bulletin of Menninger Clinic, 57, 450-457.
Strachey, J. (1934, 1969). The nature of the therapeutic action of psychoanalysis. International Journal of Psycho-Analysis, 50, 275-291.
Strupp, H. H. (1989). Can the practitioner learn from the researcher? American Psychologist, 44, 717-724.
Swift, W. J. & Wonderlich, S. A. (1990). Interpretation of transference in the psychotherapy of adolescents and young adults. Journal of the American Academy of Child and Adolescent Psychiatry, 29, 929-935.
Tanzilli, A., Muzi, K., Ronningstam, E., & Lingiardi, V. (2017). Countertransference when working with narcissistic personality disorder: An empirical investigation. Psychotherapy Theory and Research Practice Training, 54(2), 184-194.
Tower, L. E. (1956). Countertransference. Journal of the American Psychoanalytic Association, 4, 224-255.
Ulanov, A. (1984). Transference/countertransference: A Jungian perspective. In M. Stein (Ed.), Jungian analysis (pp. 68-86). Northwestern University Press.
Viederman, S. (1974). Interpretation in the analytic space. International Review of Psychoanalysis, 1, 467-480.
Weiss, J., & Sampson, H. (1986). The psychoanalytic process. Guilford Press.
Westen, D., & Gabbard, G. O. (2002). Developments in cognitive neuroscience: II. Implications for theories of transference. The Journal of the Psychoanalytic Association, 50, 99-134.
Westen, D. (1998). The scientific legacy of Sigmund Freud: Toward a psychodynamically informed psychological science. Psychological Bulletin, 124, 333-371.
Wilkinson, M. (2003). Undoing trauma: contemporary neuroscience. Journal of Analytical Psychology, 48, 235-243.
Williams, S., Shook, B., & Parker, J. (2016). Assessing marriage and family therapy graduate students’ response to sexual attraction in therapy. Psychology, 7, 258-270.
Winnicott, D. W. (1960). Countertransference. British Journal of Medical Psychiatry, 33, 17-21.
Winnicott, D. W. (1965). The maturational processes and the facilitating environment. International Universities Press.
Winnicott, D. W. (1971). Playing and reality. Tavistock.
Winston, A., McCullough, L., & Laikin, M. (1993). Clinical and research implications of patient-therapist interaction in brief psychotherapy. American Journal of Psychotherapy, 47, 527-539.
Wittig, R., Nessling, M., Will, R. D., Mollenhauer, J., Salowsky, R., Munstermann, E., Schick, M. Helmbach, H., Gschwendt, B., Kom, B., Kioschis, P., Lichter, P., Schadendorf, D., & Poustka, A. (2002). Candidate genes for cross-resistance against DNA-damaging drugs. Cancer Research, 62(22), 55-63.
Wolstein, B. (1996). The analysis of transference as an interpersonal process. American Journal of Psychotherapy, 50, 499-509.
Wrye, H. K., & Welles, J. K. (1989). The maternal erotic transference. International Journal of Psycho-Analysis, 70, 673-684.
Zilcha-Mano, S. (2017). Is the alliance really therapeutic? Revisiting this question in light of recent methodological advances. American Psychologist, 72(4), 311-325.


 ContinuingEdCourses.Net is approved by the American Psychological Association (APA) to sponsor continuing education for psychologists. ContinuingEdCourses.Net maintains responsibility for this program and its content.
ContinuingEdCourses.Net is approved by the American Psychological Association (APA) to sponsor continuing education for psychologists. ContinuingEdCourses.Net maintains responsibility for this program and its content. ContinuingEdCourses.Net, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027.
ContinuingEdCourses.Net, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027. ContinuingEdCourses.Net has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs.
ContinuingEdCourses.Net has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs. ContinuingEdCourses.Net is recognized by the New York State Education Department's State Board for Psychology (NYSED-PSY) as an approved provider of continuing education for licensed psychologists #PSY-0048.
ContinuingEdCourses.Net is recognized by the New York State Education Department's State Board for Psychology (NYSED-PSY) as an approved provider of continuing education for licensed psychologists #PSY-0048.